
Traffic to Massy |

Hotel Mercure |
Introduction I came
back to Paris, France by taking the JL405 flight departing at
11:30 AM from Narita Airport on June 24 Thursday, 2004 in order
to attend the 5th European Workshop on Transradial Approach for
Coronary Diagnosis and Interventions as one of the invited Faculty
members and operators. The workshop was held in Massy, which is
the town located at the south of Paris. I arrived at Charles
de Gaulle International Airport after 12 hours’ flight, which
is located at the north of Paris. The flight was delayed by about
30 minutes as always and arrived at 5:30 PM. I took a car from
the airport to Massy. The roads were congested because many people
went in and out from Paris. After more than 1 hour’s drive, I
checked in the hotel, Hotel Mercure Paris
Sud/Massy Gare TGV. As you can know from the name of the hotel,
it is located just beside the TGV station. The workshop was supposed
to be held from 7:00 PM in the 1st floor of the hotel, and I arrived
just at 7:00 PM. However, the actual schedule was delayed by almost
1 hour. After putting my luggage in my room, I dropped at the
1st floor, where many of attendants were already drinking and
talking with each other in the elevator hall. I found Dr. Yves
Louvard and said to him, “Hello!” He replied to my, “Welcome to
Europe.” I suddenly understood that I was alone in Europe and
accepted as a friend. I joined the group and asked to Dr. Ferdinand
Kiemeneij and Dr. Josef Ludwig, “We are waiting for somebody coming?
Why the schedule is delayed?” Their answer was interesting. That
was “No, we are not waiting for somebody. We are just waiting
for waiting. It’s French style.”
Soccer Slide |

Josef’s Speech |
The workshop was commenced by the short opening
speech by Dr. Yves Louvard, who is the Course Directors of this
Course with Dr. Thierry Lefevre. In the opening speech, he said,
“Welcome to this beautiful town, Massy!” Dr. Jean Fajadet sitting
in the left side of me whispered to me, “I am not sure whether
Massy is really beautiful or not.” The workshop was going in a
very friendly atmosphere. Everybody there was strong already strong
Radialists or young physicians who wished to be them.
The first half of the program was “Debate session”.
Since all of European people were excited about the international
soccer league, Euro2004, which was on going, all of the lectures
in the debate session were started by the slide of the national
soccer team as well as the music of the national anthem of the
nation of each speaker . The 1st speaker was Dr. Josef Ludwig
from Germany. He argued that the radial artery access should be
much better than the ulnar artery access. The opponent was Dr.
Valdesuso from Spain. He argued that the ulnar artery was quite
useful as a route of PCI as well as the radial artery. His argument
was based on his personal experiences on the consecutive more
than 200 patients with transulnar coronary intervention. This
debate was followed by the other 3 topics of debates: “Transradial
approach should be only for PCI OR for diagnosis and PCI?”, “Dedicated
hemostatic devices OR Simple elastic bandage?” and “Right radial
approach OR left radial approach?”

Having Dinner |

Dinner Food |
During the heated debates, all of the attendants
had drinking and dinner. The food was buffet style but very nice.
Since it was already 11:00 PM, I returned to my room while the
meeting was continuing. I attempted to connect my computer to
Internet. However, it seemed difficult. Then, I decided not to
connect my computer with Internet for the following 3 days.
June 25 Friday, 2004

Massy Gare TGV |

Massy Opera Building |

Meeting Entrance |
As always, I was sick for jet lag. I waked up
at 3:00 AM (= 10:00 AM in Japan Standard Time). I turned on my
computer and prepared for my presentation. It was already bright
outside at 6:00 AM. I decided to walk around the hotel and found
the TGV station. The TGV station was not only the station building
but also something like a modern art . I again understood that
I was now in France. I had been informed that the bus to the Venue
of the live demonstration would start between 7:15 and 7:30 AM.
I checked out the hotel and had a light breakfast. Josef was smoking
a cigarette in front of the hotel. I came to him and said, “Good
morning!” Josef told me that he had seen my website describing
my visits in Paris and Moscow. He asked to me, “Have you taken
the photos of beautiful scenery around the hotel for your web
site?” Of course, the answer was “Yes!”
Many people said, “It is France.” The bus came
to the hotel around 7:40 AM. It took just only 5 minutes to the
venue of the live demonstration, “Massy Opera” . It is a kind
of public theater. We used a medium-sized theater room. At the
entrance of the theater, there was the sign curtain of the meeting.
The hospital, where live cases were performed, is located at the
opposite side of the parking space and just only 2 minutes’ walk
distance from Massy Opera.

Hospital |

Live Case Transmission |
The program was well organized. It started at
8:00 AM by the opening short speech of Dr. Thierry Lefevre, and
was followed by 2 live demonstrations of transradial diagnostic
coronary angiographies. The 1st case was done through the right
radial approach by one fellow doctor under Yves and finished very
smoothly. The 2nd case was done through the left radial approach
by Dr. Monsegu, who argued last night that the left radial approach
was much better than the right and are the consultant Cardiologist
in the Military Hospital of Paris. However, it took long time
to get the successful engagements of the catheters into the coronary
arteries. Ferdinand’s comment in the auditorium was so witty.
He said, “You are so kind to show us all of the disadvantages
from the left radial approach.”
Following these 2 live cases, Dr. Blanchard made
a lecture: “Why I became the Radialist, after my more than 20
years’ history as a Femoralist.”
The 3rd live case was performed by Dr. Urban from
Switzerland. He is an expert Interventional Cardiologist but has
not so much experiences in TRI. His case was a patient with the
bifurcation lesion in the mid-LAD and the 1st diagonal branch.
He did an excellent bifurcation stenting using 2 TAXUS DES stents
following the excellent teaching from Yves, who was standing beside
Dr. Urban during his procedure. France has a strict national regulation
for foreign doctors to do cases. Any doctor even from EU countries
cannot do medical practice, if the expert French doctor is not
standing beside him in front of the patients.
Next lecture was made by Dr. Spaulding. He is
very famous in this field. I was really impressed to see him first
time. He did an important lecture about the medical treatment
during TRI. After 15 minutes’ coffee break, Dr. Hildick Smith
made a lecture on their OCTOPLUS study, in which they tested the
superiority of TRI over TFI among the elderly patients >= 80
years old. As I you can guess, his conclusion was, of course,
that TRI is better than TFI.
Dr. Gerald Barbeau from Quebec City, Canada was
asked to do a very difficult case. The lady patient had previous
stenting in LCX and RCA. The target lesion this time was located
in the middle part of heavily calcified LAD. He showed a 6 French
Sheathless guiding catheter system. Beside him, Yves was standing
and said to Gerald, “We arranged this case for you, because we
know you are a very skillful operator.” The case was really difficult
and took long time. In the meantime, Yves left that laboratory
and moved to the other laboratory. The screen was switched to
the case done by Yves. His case was the patient with in-stent
restenosis just at the ostium of LAD. He did a beautiful stenting
from LMT to LAD by using a TAXUS DES stent followed by the simultaneous
kissing balloon dilatation. After the finish of Yves’s case, Thierry
did a short quiz-style lecture regarding the anatomy of the radial
artery. Following his lecture, all of the attendants moved to
the next room to have a lunch together. I sat at the table with
doctors from Bulgaria and people from Switzerland. We talked a
lot with each other. Last night, we learnt a lot about the status
of PCI and TRI in Europe. The penetration rate of TRI in France
exceeded 36% in whole nation last year and is expected to be more
than 45% this year. The penetration rate of TRI is rapidly growing
in all of the European countries. Among them, German was different.
However, Josef did an interesting speech. “German Government announced
that the diagnostic coronary angiographies will not be reimbursed
from next year, if it is not done by outpatient basis. After this
statement, all of the Femoralists in Germany are now trying to
learn the transradial approach

Dr Alenxander Doganov wearing a blue shirt |
.” Dr. Alexander Doganov is the director of the
catheter laboratory in National Heart Hospital of Bulgaria in
Sophia. In his presentation last night, he showed that almost
50% of the cases were done through TRI among >= 1,100 cases
of PCI cases last year in his hospital. A Hungarian doctor also
reported that more than 50,000 cases of PCI were performed last
year in Hungary. This number is quite amazing. It is almost similar
to the numbers in UK or Italy and probably more than in China.
I asked to Alexander, “Why the case numbers are so rapidly growing
in middle European countries?” His answer was, “Because of high
incidence of smoking and food style. Of course, the economy has
grown up rapidly in these several years. That is the main reason.”
According to Alexander, the GDP in Bulgaria surprisingly increased
by 3 times since 2002. During the lunch, 2 bottles of French Red
Wine were served in each table. I drank up 4 glasses of it.
The afternoon session was started by Gerald’s
report about his case. Gerald did an excellent job. All of the
severe dissections created by balloon dilatation in the calcified
LAD were repaired by the implantation of 3 Driver stents and 1
TAXUS stent. Next lecture was done by Dr. Orazio Valsecchi from
Italy about TRI for AMI patients. I already published an article
about my TEMPURA trial, where the AMI patients were randomly assigned
to either TRI or TFI [Saito S, et al. Comparative study on transradial
approach vs. transfemoral approach in primary stent implantation
for patients with acute myocardial infarction: results of the
test for myocardial infarction by prospective unicenter randomization
for access sites (TEMPURA) trial. Catheter Cardiovasc Interv.
2003; 59: 26-33.).
After his lecture, Ferdinand did his live case.
Thierry was standing beside him. His case was a young diabetic
gentleman who had previous stenting in proximal LAD and RCA 3
or 4 years ago without any subsequent instent restenosis. The
target lesions this time were tandem tight lesions in the distal
LAD. The discussion proposed by him was whether DES should be
used or not in these distal LAD lesions in a diabetic patient
who had previous BMS stent implantation previously without any
subsequent instent restenosis. According to Ferdinand, any DES
is not reimbursed by the insurance in Holland. Thus, if DES is
used for the patient, either the doctor or the hospital has to
pay for that DES. I know that they were using DES stents in all
of the cases in Thoraxcenter, Rotterdam, where I did my live case
there in the last EuroPCR meeting. I asked Ferdinand, “Why they
are using 100% DES in Rotterdam?” His answer was, “Because they
are doing a good negotiation with a company.” Actually, in OLVG
hospital, Ferdinand is using DES stents only in less than 20%
of stent implantation cases. Because Thierry strongly advised
him to put DES stents in that patient, he finally placed 2 TAXUS
stents. By the way, Orazio informed me that DES was interestingly
reimbursed only for 25% of the price by the insurance system in
Italy.
After Ferdinand finished his case successfully,
I was asked to do my lecture. My lecture title was “TRI for CTO
lesions”. Since the lecture time was limited to 10 minutes, I
condensed my presentation. After my presentation, Yves said, “We
learnt a lot about CTO in these 10 minutes.”

Hospital Entrance |
I asked Yves to take me to the hospital. The hospital
was “Institut Hospitalier Jacques Cartier”. The hospital is a
private hospital run by a big hospital management company in France.
Drs Yves Louvard, Thierry Lefevre and Marie Claude Morice have
an independent Cardiology section, “Institut Cardiovasculaire
Paris Sud (= South Paris Cardiovascular Institution)”, within
the hospital. They invested 50% of the capital for the Cardiology
section, and the remaining 50% of the capital were paid by the
hospital company. Yves watched my live case transmissions of successful
PCI for CTO lesions during Nagasaki Live Demonstration on June
6 and Moscow
Live Demonstration on June 08. He sent me an e-mail for the
possible candidate for my live case on June 12. The case was a
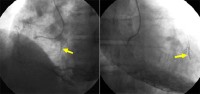
68 y.o. male patient with previous anterior myocardial infarction.
Coronary angiogram showed a tight narrowing in the big high lateral
branch, which was though to be the culprit lesion for the current
effort angina, and a chronic total occlusion in the middle LAD.
In the e-mail, Yves asked me whether the case would be OK or not
for me. I replied, “Yes, the case is OK. However, could you accept
my possible failure in PCI?” The Cardiology section was located
in the 3rd floor, which consisted of 3 catheter laboratories,
a patient care room for the patients before and after the procedures,
and several rooms. I changed my clothes in the room, which might
be Dr. Morice’s room. When I came in the catheter laboratories,
Thierry was doing a live case transmission. The case was a patient
with left main bifurcation stenting after bypass surgery.

RAO Cranial |
RCA |
LAO Cranial |
Because it was already behind the schedule, I
was asked to start the radial artery puncture in the off-line
setting. It was lucky for me that the patient’s right radial artery
was big. I inserted a 6 French semi-long TERUMO introducer successfully
and took a 6 French EBU4.0 guiding catheter (Launcher, Medtronic).
In the meantime, Thierry came in the room and stand beside me,
after he finished his case. The patient’s left main artery was
short, and the guiding catheter easily wedged into the coronary
ostium, whenever I tried to direct the tip of the guiding catheter
for LAD. The patient had already stent implantation in the critical
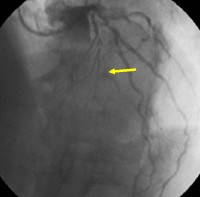
narrowing in the diagonal branch several days ago. The left anterior
descending artery distal to the occlusion was clearly visualized
from RCA but faintly from LCX. I wondered from which point the
main LAD branched away. There were 2 possibilities. One was at
the 1st major septal branch, and another was at the 2nd distal
branch. Anyway, everybody in the auditorium and the catheter laboratory
as well as me thought that it might be impossible to open this
occlusion. First, I took a Magic-FA guidewire together with a
Transit microcatheter and searched for any catch of the tip of
the guidewire by a invisible notch within the artery, and then
finally I was convinced that the entry point should be at the
2nd major septal branch but not at the 1st one. Since I felt that
the Magic-FA guidewire was too weak to make a hole at the notch,
I exchanged it to a Conquest guidewire. However, the Conquest
guidewire was too poor in torque controllability to direct the
tip against the notch. Thus, I again exchanged the guidewire with
a Magic-Ex guidewire. This guidewire was enough in torque controllability
for creating a shallow hole at the notch, although it could not
advance anymore. Finally, I replaced the guidewire by a Conquest-Pro
guidewire. Since there was a shallow hole at the notch site within
the artery, the Conquest-Pro guidewire gradually advanced into
the possible occlusion site. While I was doing these procedures,
Jean was fighting against a difficult lesion in the ostium of
the saphenous vein graft to LAD. And, the screen in the auditorium
was televising his procedure. Responding to Thierry’s call, the
screen came to me. I explained the procedures, which I did before,
and continued it. The guidewire finally came into the distal true
lumen. I inflated the occlusion site by a 1.5-mm Maverick balloon
(Boston Scientific), followed by the 2.5 x 30 mm balloon inflation.
Everybody in the auditorium and the laboratory was very surprised
to see the results. Thierry made a short comment, which was very
impressive for me. It was, “I think there are 2 doctors in the
world, whose skill is very excellent. They are Dr. Saito and Dr.
Kato.” It was really a great honor for me to hear this comment.
I also really appreciate for Yves’ comment. It was, “I saw Dr.
Saito was doing PCI for CTO lesions in Nagasaki and Moscow.
All of the cases were successful. Thus, I believe that today’s
success is possible not by a chance, but definitely by his skill
and experiences.”

Our Team |

Entrance of Massy Opera |

Hors D’oeuvre |

Yves |

Ferdinand |
Since the scheduled transmission time was almost
over, Thierry called the patients, who had procedures during the
transmission in the morning, into the catheterization laboratory.
They walked in on their foot. It was really impressive, since
these demonstrations clearly showed the advantages of the transradial
approach in comparison with the transfemoral approach. Because
the patients were not wearing X-ray protectors, I had to stop
the procedures. After the patients left the room, I placed a 2.5
x 32 mm Cypher stent in the middle of LAD and a 2.75 x 28 mm Cypher
stent in the proximal part of the 1st stent with 1-strut overlapping
manner. I was very happy for the results as well as Thierry and
all of the nurses. The nurses praised me for this success. Thierry
said to me, “It is really valuable and difficult to draw applause
from such expert nurses.” After finishing this case, our team
took a memorial photo together.
I returned to the auditorium alone by myself.
The meeting was finished soon. After the adjournment, several
of the faculty members visited the office of the Institut Cardiovasculaire
Paris Sud to cerebrate the great success of this meeting together
with Yves. The office was at the 3rd floor of the building opposite
to the Massy Opera. There were bottles of champagne and dishes
of hors d’oeuvre arranged. Yves opened the champagne bottles,
and I had glasses of champagne with Ferdinand. Ferdinand said
to me, “Yves is always assigned to do live cases for bifurcation
lesions, and you are always for CTO lesions. They are your fate.
I will arrange you a patient with type-A simple lesion during
my Amsterdam Live Demonstration in October.”

Hotel Royal Barriere |

Entry of Hotel Royal Barriere |

Casino Barriere de Deauville |

Casino Barriere de Deauville lightened |
Because I had to go to Deauville to meet Dr. Martial
Hamon that night, a taxi was waiting for me at 6:00 PM in front
of the auditorium. I took the taxi, after I said to everybody,
“Good By and See you again!” While I was sleeping in the taxi,
it arrived at Hotel Royal Barriere de Deauville 3 hours later.
The building is very elegant and beautiful. It was already 9:00
PM. I moved to the restaurant within Casino Barriere de Deauville.
There Martial and many Cardiologists were having dinner together.
I sat in the seat next to Martial. The dinner was arranged during
the Symposium for Hear Failure. This Symposium was sponsored by
CHU de Caen (Caen University Central Hospital), and the famous
doctors from Boston or Montreal were invited. Because Martial
is responsible for the academic activities in the field of Cardiology
within CHU de Caen, he was the organizer of this Symposium, and
it was the reason why he could not join the Massy TRI meeting
this year. When Yves knew that Martial could not attend the meeting,
Yves was really disappointed. The dinner was finished by 10:30
PM, and all of us moved to the Theater next to the Restaurant.
A nice French dancing and musical show entitled “Elles” started
from 10:40 PM.
We sat together, drank glasses of champagne
and watched the show. The show was fantastic. I watched it by
its final stage despite my severe jet lag. I came back to my hotel
room later than 0:15 AM. It was a really long day for me.

Ticket for Elles |
Elles |
June 26 Saturday, 2004

Entry of Centre International Deauville |

Discussion in the Symposium |

Normandie Coast |
Map of Deauville |
I visited Deauville in order to have filming my
introduction for the Web Site and CD-ROM directed by Martial.
This Web Site and CD-Rom are focusing on 5 French guiding catheters
through TRI. During the
last EuroPCR meeting, Martial asked to me to came to Deauville
for the filming. At 10:00 AM, I met with a gentleman from the
filming company. He took me to the convention center named as
“Centre International Deauville”, where the famous American Film
Festival is held every autumn. It was just at 3 minutes’ walk
distance from my hotel. Filming was smoothly finished in 30 minutes.
Since the Symposium for Heart Failure was held within the convention
center, I joined the Symposium after the filming. I could understand
the lecture slides, although I could not understand the discussions,
because they were done only in French . After I stayed in the
Symposium for 30 minutes, I decided to leave the Symposium and
walk around this beautiful town alone by myself.
Deauville is a small beautiful town along the
sea coast in Normandie.

Gucci |

Polo-Ralph-Lauren |

Longshamp |

Hermes |

Dior |

Ferragamo |
Deauville is one of the famous resorts for French
people living in Paris, so that many famous boutiques are there
. Since I visited this town last
year, I knew the area. Both Hotel Normandie and Hotel Mairie
are typical old buildings in Deauville .

Hotel Normandie |

Hotel Mairie |
I walked to the next town, Trouville. A small
river is separating these 2 towns. Trouville is also a beautiful
town. It is originally not a Resort town but a fisherman’s town.
Because of that, there are several shipyards. However, because
next town Deauville became famous for tourist, Trouville is now
also accepting many tourists. There is also Casino Trouville .
Hotel de Ville is a good landmark because of its highest building
within the town. There are many small seafood restaurants . We
have to cross a bridge to move between Deauville and Trouville.

The Rive |
Map of Trouville |

Shipyard |

Casino Trouville |

Hotel de Ville |

Street in Trouville |

End of Deauville |

End of Trouville |

La Marine |

Marche de Poisson |

Fishes |

Moules Mariniere |
While I was walking around, I met several Korean
families but not any Japanese tourists. The reason why I did not
see any Japanese tourists, I guessed, was because Japanese tourists
travel everywhere as a group together and not as families. I felt
that Korean were more independent than Japanese. However, I knew
it was not a reason. I found the true reason later. It was already
at noon time, and I was hungry. I dropped in a seafood restaurant.
It is “La Marine” and located just in front of the fish market,
“Marche de Poisson”. We can see many kinds of ocean fishes there.
I sat alone at the table outside the restaurant. It might seem
curious for the other people to see that an oriental man with
a suit and tie was sitting alone in the restaurant. I ordered
one of my most favorite foods in France, “Moules Mariniere” together
with a cup of fish soup and a plate of boiled langoustines.

Sopes de Poissons |

Langoustines Mayonnaise |
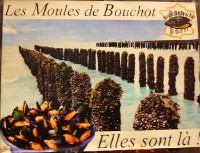
Les Moules de Bouchot |

Menu |
A blue mussel “Moules” is very famous in this
area. It is now cultured in the coast. The special culture for
“Moules” is called “Bouchot”. The total price together with a
half battle of Chablis Premium was about 65 Euros. The taste was
so excellent that I recommend you to visit this Brasserie Restaurant
if you visit Trouville. While I was waiting for foods coming,
a group of oriental men came in the restaurant. They were a TV
crew. One of them was bringing a TV video camera. Surprisingly,
I could see the label of KBS (=Korean Broadcasting Service company)
on the camera. I got it. Because TV programs for tourism in Korea
are now telecasting this area, there are many Korean tourists.
After finishing the lunch, I walked back to Deauville.
I was surprised to see the signboard of “NAUSICA” at a Brasserie.
However, I found soon it was “NAUTICA”. On the way back to Hotel
Royal Barriere, I found a station. The name of the station is
a buddy name. It is “Gare de Trouville-Deauville”.

Brasserie NAUTICA |

Trouville-Deaville Station |

Taxi |

La Saine |
After saying “Good-by“ to Professor Hamon at the
hotel, I went back to Paris by a taxi. We crossed the border of
Paris along the river “Saine”. It is a beautiful river. A girl
was water skiing. I finally arrived at Charles de Gaulle International
Airport before 5:00 PM. I took an ANA flight and came back to
Japan on June 27 Sunday, 2004.
Anyway, this travel was my 1st experience alone
in European people. I was really impressed to know again that
they are really kind and friendly. Thank you so much for their
kindness. Also, this was my 1st experience for not connecting
my computer with Internet for as many as 3 days in the past 7
or 8 years.
Hints in France

Gasoline Price |
The gasoline price in France is more expensive
than in Japan. The price for 1 litter of normal gasoline is almost
140 Japanese Yen. We can see frequently the sign of “Barriere”
in Deauville. It is the name of the hotel group, “Lucien Barriere”.
They have Casino and 2 hotels in Deauville.
フランス訪問記- II
湘南鎌倉総合病院 心臓センター循環器科
齋藤 滋
はじめに
Traffic to Massy |
Hotel Mercure |
2004年6月24日成田午前11:30発のJL405便に乗って、経橈骨動脈冠動脈造影および冠動脈インターベンションに関する第5回ヨーロッパ・ワークショップに招聘術者・講師として出席するために再びパリに戻りました。このワークショップはMassyで開催さました。Massyというのはパリ郊外南にある小さな町です。出発が毎度のことで30分ぐらい遅れたので、12時間の飛行の後にシャルル・ド・ゴール国際空港に到着したのはかれこれ午後5時30分でした。自動車でMassyに移動しましたが、パリから出る人、帰る人で道路は渋滞していました。1時間以上のドライブの後にHotel
Mercure Paris Sud/Massy Gare TGVにチェック・インしました。名前の通り、このホテルはTGVの駅のそばにあります。ワークショップは午後7時からホテル1階(但し、フランスでは通常フロントがある階を0階と称するので、日本で言えば2階に相当)で開催される予定であり、私が到着したのも同時刻でした。しかし、実際の開催はかれこれ1時間も遅れました。部屋に荷物を置いた後、1階に降りて行くと、既にたくさんの人が飲んだり喋ったりしていました。Yves
Louvard先生を見つけたので、「こんにちは」と、声をかけると、彼は私に、「ようこそヨーロッパへ」と、言われました。それで気づいたのですが、「自分は今、ヨーロッパに一人でいる。そして、皆から友人として迎えられた。」それからFerdinand
Kiemeneij先生とJosef Ludwig先生のグループに加わりました。そして、「誰か来るのを待っているのかな? どうして遅れているのかな。」と、聞きました。その答えは面白かったです。それは、「違うよ、誰も待っていないよ。ただ待つために待っているんだよ。これがフランスさ。」
Soccer Slide |
Josef’s Speech |
ワークショップはYves Louvard先生の短いオープニング・スピーチと共に始まりました。彼は、Thierry
Lefevre先生と共に、この会のコース・ディレクターです。そのスピーチの中で、彼は「この美しい町、Massyにようこそ」と言われました。僕の左隣に座っておられたJean
Fajadetが私に囁きました。「本当かね、Massyって綺麗な町かな」ワークショップは非常に和んだ雰囲気の中で進行しました。参加者皆は既に熱烈なるRadialistである、あるいはそうなりいと強く思っている若い先生方ばかりでした。
プログラムの前半は、ディベィト・セッシヨンでした。ちょうど、ユーロ2004というサッカー・リーグが開催されていたこともあり、ヨーロッパの人々は皆サッカーに興奮していました。このためもあり、このディベート・セッションでの講演は全て演者の国のサッカー・チームのユニフォームのスライドと国家の演奏で始まりました。
最初の演者はドイツからのJosef Ludwig先生でした。彼は、橈骨動脈アプローチは尺骨動脈アプローチよりもはるかに優れていると、主張しました。スペインのValdesuso先生は自分自身の連続200例以上の経尺骨動脈冠動脈インターベンションを行った患者さんの経験に基づいて、尺骨動脈アプローチはPCIのルートとして有用であると、主張しました。これに引き続いて、「橈骨動脈アプローチはPCIのためだけに用いるべきか、あるいは診断カテーテルにも用いるべきか」、「止血には専用の止血器具を用いるか、あるいは普通の弾性絆創膏で良いか」そして「右橈骨動脈あるいは左橈骨動脈」という3つのディベートが行われました。
Having Dinner |
Dinner Food |
活発なディベートの間、参加者は飲み、食べました。食事はセルフ形式で、とてもおいしいものでした。もう時刻も午後11:00時となっていたので、会は未だ続いていましたが私は部屋に戻りました。そして、コンピューターをインターネットに継ごうとしたのですが、とても困難に感じでした。それで、もうこれからの3日間はインターネットに継げるのをやめることに決めました。
2004年6月25日金曜日
Massy Gare TGV |
Massy Opera Building |
Meeting Entrance |
毎度の如く、私は時差ぼけでした。日本時刻午前10時にあたる現地時刻午前3時に目がさめました。そしてコンピューターのスイッチを入れて、自分の発表の準備をしました。午前6時になると既に外は明るくなっていました。そこで、ホテルの周りを歩いてTGVの駅を探しに行くことにしました。TGVの駅は単なる駅というよりもモダン・アートのようなビルでした。そんな訳で、「やっぱりフランスにいるんだ」と、思いました。ライブの会場に行くバスが午前7時15分から30分の間にホテルの前を出ると言われていました。チェック・アウトを終えてから軽く朝食を食べました。Josefがホテルの前でタバコを吸っていました。「お早う」と彼に呼びかけました。Josefは僕のWebsiteの中のモスクワ編とパリ編を見たよ、と僕に言いました。そして、「Websiteに載せるために、この周りの綺麗な景色を写真撮った?」と僕に聞きました。もちろん、「そうさ」と、答えました。
皆が「これがフランスさ」と、言いました。バスは7時40分頃来ました。ライブ会場のMassy
Operaまでは5分足らずでした。この建物は一種の公共劇場です。私たちはその中の中くらいの部屋を使いました。劇場の入り口には会の垂れ幕がかかっていました。ライブ手技が行われ病院は駐車場を隔てて向かい側にあり、Massy
Operaからは歩いてほんの2分の距離でした。
Hospital |
Live Case Transmission |
プログラムは良くできたものでした。Thierry Lefevre先生による短い開会の挨拶に引き続いて、2例の経橈骨動脈診断冠動脈造影がライブ中継されました。第1例目は、Yves先生のところの研修医によって右橈骨動脈アプローチによって行われ、スムーズに終了しました。第2例目はMonsegu先生が術者で左橈骨動脈アプローチによって行われました。Monsegu先生は昨夜、左橈骨動脈アプローチが右橈骨動脈よりもずっと良いと主張された先生であり、パリ軍病院の循環器内科医です。でも、冠動脈へのカテーテル挿入には大層な時間がかかりました。Ferdinandは会場で面白いコメントをしました。それは、「君は何て親切なんだい。だって、左橈骨動脈アプローチの欠点を全て皆の前にさらけ出してくれているんだから。」
この2例のライブ中継に引き続き、Blanchard先生による「20年間もFemoralistだったのに、何で私がRadialistに転向したか?」という講義が行われました。
ライブ3例目はスイスのUrban先生によって行われました。彼はとても優秀なInterventional
Cardiologistですが、TRIに関してはあまり経験がありません。彼の症例は左前下行枝と対角枝の分岐部病変でした。YvesがUrban先生の横に立って適切な指示を与え、彼はそれに従って2つのTAXUXステントを用いて素晴らしい分岐部ステント植え込みをしました。フランスでは外国医師が手技を行うことに関して厳しい法律的制約があります。EU諸国の医師ですら、それがどんな医師であれ、フランス人の医師が患者さんの前で横に立っていないと手技は出来ません。
次の講義はSpaulding先生によるものでした。彼はこの分野でとても有名です。初めて彼を見てとても感激しました。彼の講義はTRIの時の投薬というとても重要なものでした。その後15分間のコーヒー・ブレークがあり、Hildick
Smith先生がOCTOPLUS研究の講義を行いました。これは80歳以上の患者さんに対するTFIに対するTRIの優位性を調べた試験です。皆の予想通り、これの結論は勿論のこと、TFIよりもTRIが優れている、というものでした。
カナダのケベック市から来たGerald Barbeau先生は大変な症例に当たりました。その女性患者さんは既に右冠動脈と左回旋枝にステントを植え込まれていました。今回の病変は非常に石灰化した左前下行枝の中部にある病変でした。彼はまずシースレスのガイディング・カテーテル・システムを披露しました。彼の傍らに立つYvesは言いました。「この症例は君に用意したよ。だって、君が優秀な術者だと知っているから。」その症例は本当に難しく、とても時間がかかりました。途中でYvesはそのカテ室を離れ、次のカテ室に移りました。そして、Yvesの行う手技に画面が切り替わりました。彼の症例は左前下行枝入口部に植え込まれたステントのステント内再狭窄の症例でした。TAXUSステントを左主幹部から左前下行枝に植え込み、その後同時キッシング・バルーンを行うことによって、非常に素晴らしいステント植え込みを披露しました。Yvesの症例が終わってからThierryが橈骨動脈の解剖に関して短いクイズ形式の講義をしました。この講義の後、皆で隣の部屋に移り、ランチを一緒に食べました。私は、ブルガリアの医師とスイスの人と一緒のテーブルに座りました。色々なことを話しました。昨夜、私たちはヨーロッパにおけるPCIとTRIの現状についてもたくさん知りました。昨年フランス全土でのTRIの施行率は36%を超えた、ということです。そして、今年は45%以上と予想されるそうです。全ヨーロッパ諸国においてTRIの浸透度は急速に上昇しています。その中で、ドイツは異色でした。しかし、Josefは面白いことを言いました。「ドイツ政府は来年から診断カテーテルは外来ベースで行わない限り保険償還しないことを発表した。この発表の後、ドイツのFemoralistは皆、慌てて橈骨動脈アプローチを練習し始めた。」というものでした。Alexander
Doganov先生はソフィアにあるブルガリア国立心臓病院のカテ室部長です。
Dr Alenxander Doganov wearing a blue shirt |
昨夜の彼の発表によれば昨年彼の病院では年間1,100例以上のPCIの内、大体50%でTRIが用いられたということです。ハンガリーの医師の発表によれば、ハンガリーでは昨年一年間に50,000例以上のPCIが行われたということです。この数はとても驚きです。この数というのは、イギリスやイタリアと同じぐらいの数ですし、中国よりも多分多いと思います。Alexanderに聞きました、「どうして中欧諸国ではそんなに吸息に症例数が伸びているの?」。これの答えは、「喫煙率が高く、食事のせいだ。もちろんこの数年で経済も急速に成長した。これが大きな理由だ。」というものでした。AlexanderによればブルガリアのGDPは2002年から何と3倍になった、ということです。昼食には、各テーブルに赤ワインが2本ずつ配られました。私は、グラス4杯開けました。
午後のセッションはGerald自身による彼の症例のその後の報告から始まりました。Geraldはとてもうまくやりました。石灰化した左前下行枝をバルーンで拡張した後できたひどい解離は全てDriverステント3つと、TAXUSステント1つの植え込みで完全に修復されました。次の講演はイタリアのOrazio
Valsecci先生によるものでした。彼のトピックは急性心筋梗塞患者さんに対するTRIというものでした。私は既にTEMPURA試験の結果を出版しています。この試験の中で急性心筋梗塞患者さんに対してTRIとTFIを無作為化しました。この結果は、CCI誌の2003年59巻26-33ページに掲載されています。
この講演に引き続いて、Ferdinandがライブを行いました。Thierryが横に立ちました。彼の症例は糖尿病を有する若い男性でした。3年あるいは4年前に左前下行枝近位部と右冠動脈にステントが植え込まれていました。今回の病変は左前下行枝遠位部のタンデム病変でした。既にBMSが植え込まれ、そのステントが再狭窄を呈さなかった糖尿病患者さんのこのような左前下行枝遠位部病変に対して、果たしてDESを用いるべきか否かについて、Ferdinandは議論を投げかけました。Ferdinandによれば、オランダではDESは保険償還されないのだそうです。ですから、もしもDESを患者さんに対して植え込んだならば、医師か病院がそのDESの費用を支払わねばならないそうです。この前のEuroPCRの時に私がライブを行ったRotterdamのThoraxcenterで全例DESを植え込んでいるのを知っていました。そこでFerdinandに聞きました。「どうしてRotterdamでは100%
DESを使っているのか?」彼の答えはこうでした、「彼らは会社とうまいこと交渉しているからさ。」実際にOLVG病院ではFerdinandはたった20%以下でしかDESを用いていないそうです。Thierryは強くDESを植え込むことを薦めました。このため、Ferdinandは最終的にTAXUS
2個を植え込みました。ところで、Orazioによればイタリアでは面白いことにDESに対してはその費用の25%のみが保険償還されるということでした。
Ferdinandがライブを終わった後、私が講演をすることになりました。講演のタイトルは「CTO病変に対するTRI」というものでした。講演時間はたったの10分間に制限されていましたので、講演内容はとても絞ったものでした。講演を終わったところ、Yvesは「この10分間で我々はCTOに対してたくさん勉強した。」
Hospital Entrance |
Yvesに病院に連れていってくれるように頼みました。病院は“Institut Hospitalier
Jacques Cartier” というものです。この病院はフランス国内で病院を運営している大きな会社によって運営されている私立病院です。Yves
Louvard先生、Thierry Lefevre先生そしてMarie Claude Morice先生の3人でInstitut
Cardiovasculaire Paris Sud(南パリ心臓血管研究所)という独立した循環器セクションを病院内に持っています。この3人で50%の資金を出資し、残りを病院が出資しているそうです。6月6日の長崎ライブデモンストレーション、そして6月8日のモスクワ・ライブデモンストレーションで私がCTOに対するPCIを上手に行ったのをYvesは自分の目で見ていました。彼は、6月12日の電子メールで私にライブで行う症例の写真を送ってきました。冠動脈造影写真は、大きな対角枝のきつい病変、これが今回の狭心症責任病変です、それと左前下行枝中部のCTO病変を示していました。Yvesは私に、「この症例で良い?」と、聞いてきました。私は、「OKだよ。でもうまくいかなくてもゴメンネ」と、答えました。循環器セクションは3階にありました。そこにはカテ室が3つあり、手技の前後の患者さんをケアする部屋もありました。私は、Morice先生の部屋とおぼしき部屋で着替えました。カテ室に入るとThierryがライブ症例をやっていました。その症例というのは冠動脈バイパス手術後の患者さんで、左主幹部分岐部病変のものでした。
RAO Cranial |
RCA |
LAO Cranial |
既に進行が予定よりも遅れていたため、予め橈骨動脈穿刺を済ましてしまうように言われました。ラッキーなことに患者さんの橈骨動脈はとても太く、6
FrenchのTERUMOセミ・ロング・シースを挿入しました。そして、6 FrenchのEBU4.0 (Launcher)を用いました。そうこうする内にThierryが自分の症例を終えてから部屋に入ってきて、私の傍らに立ちました。患者さんの左主幹部はとても短く、ガイディング・カテーテルを左前下行枝に向けようとすると、すぐに冠動脈入口部にウェッジしてしまいました。数日前に対角枝病変はステント植え込みで治療されていました。左前下行枝の閉塞部末梢は右冠動脈から良く造影されましたが、左回旋枝からもかすかに造影されていました。どの部分から閉塞部が始まるのか分かりませんでした。可能性は二つだと思いました。一つは第1中隔枝の部分、もう一つは第2中隔枝の場所でした。何れにしても、会場の皆およびカテ室内の人々、そして私自身も「こりゃあー、とっても無理だ」と、思いました。まず、Transit
+ Magic-FAで入りました。そして、動脈内の見えない窪みを探りました。そして、最終的に第2中隔枝の部分がエントリーであると確信しました。Magic-FAはこの窪みに穴を掘り込むためには弱すぎると思われたのでConquestに交換しました。しかし、この窪みに対して穴を掘り込むには、このConquestはトルクが弱すぎます。そこで、今度はMagic-Exに交換しました。このガイドワイヤーはトルクがとても強いので、窪み部分に浅い穴を掘り込むことが出来ましたが、進むことはできませんでした。次いで、Conquest-Proに交換しました。既に窪みに浅い穴が掘り込まれていましたので、このガイドワイヤーは閉塞部を進んで行きました。私がこれらの手技を行っている一方でJeanは左前下行枝への大伏在静脈グラフト入口部のとても難しい病変と格闘していました。そして、会場のスクリーンはその症例を放映しました。Thierryの呼びかけに応じてスクリーンは私の方に来ました。私はこれまでに何をやってきたかを説明しながら続けました。ようやくガイドワイヤーは閉塞遠位部の真腔に入りました。閉塞部を1.5mmのMaverickバルーンで拡張後、2.5
x 30mmのバルーンで拡張しました。会場の皆もカテ室の皆もこれを見てとても驚いていました。とても印象的なコメントをThierryがしました。「私は、とってもうまい術者が世界に2人いると思う。それは齋藤 滋先生と加藤 修先生だ。」というものでした。このコメントは私にとってとても誇るべきものです。また、Yvesのコメントもとても嬉しいものでした。それは、「長崎、そしてモスクワで齋藤 滋先生がCTOに対してPCIを行うのを見ました。そして、その全てが成功しました。だから、今日の成功も単なる偶然ではないと思います。この成功は間違いなく、彼の技術と経験に裏付けられたものです。」
Our Team |
Entrance of Massy Opera |
Hors D’oeuvre |
Yves |
Feridnand |
もうライブ予定中継時間は終わりに近づいていました。そこでThierryは午前中にライブで手技を受けた患者さんたちをカテ室に呼び寄せました。彼らは歩いてカテ室に来ました。この光景はとても印象深いものでした。本当にTFIよりもTRIが優れていることを示すものでした。患者さんたちはレントゲン防護服を着ていませんでしたので、私としては手技を止めざるを得ませんでした。患者さんがカテ室から出た後、2.5
x 32mmのCypherステントを左前下行枝の中部に植え込みました。そして、このステントと少し重なるようにして2.75 x
28mmのCypherステントを植え込みました。結果にはカテ室内の看護婦さん達もとても喜びました。Thierryは僕に言いました、「彼女たちのような熟練した看護師達から賞賛を得るのは本当に難しいんだよ。」この症例を終えてから私たちは記念写真を撮りました。
一人で会場に戻りました。会はすぐに終わりました。終了後、ファカルティー数名が集まり、南パリ心臓血管研究所の事務室に集まり、Yvesと共に会の成功を祝いました。事務所はMassy
Operaの向かいのビルの3階にありました。そこにはシャンパンの瓶と、オードブルが並べられていました。Yvesがシャンパンを開け、私はFerdinandと共に頂きました。Ferdinandは言いました、「Yvesは何時だって分岐部病変の症例を割り当てられるし、君は何時だってCTOの症例を割り当てられる。それが運命さ。今度の10月のAmsterdamでのTRIライブの時には、Type-Aの簡単な症例を割り当てるさ。」
Hotel Royal Barriere |
Entry of Hotel Royal Barriere |
Casino Barriere de Deauville |
Casino Barriere de Deauville lightened |
その夜はDeauvilleに行き、Martial Hamon先生と会わねばなりませんでしたので、タクシーを会場の入り口に午後6時に待たせていました。皆に、「さよなら、またね」と言った後、タクシーに乗りました。眠っている間にタクシーは3時間かけてRoyal
Barriere de Deauvilleホテルに到着しました。既に時刻は午後9時。私はすぐにCasino Barriere
de Deauvilleに移動しました。そこではMartialとたくさんの循環器内科医が一緒に夕食を摂っていました。Martialの隣に座りました。この夕食会は心不全のシンポジウムの一環として企画されていました。シンポジウムはCaen大学病院の主催で開催され、BostonやMontrealの有名な先生方が招かれていました。MartialはCaen大学病院での、循環器領域学術委員をしているのでこのシンポジウムを実際に執り行わねばなりませんでした。ですから、Martialは今回のMassyには参加することができず、Yvesはとても残念がりました。夕食は午後10時30分までに終了し、我々は皆でレストランの隣の劇場に移動しました。
そこでは午後10時40分から如何にもフランス的なミュージック”Elles”が行われていました。ショーはとても素晴らしかったです。最後まで見てから、午前0時15分過ぎにホテルに戻りました。とっても長い一日でした。
Ticket for Elles |
Elles |
2004年6月26日土曜日
Entry of Centre International Deauville |
Discussion in the Symposium |
Normandie Coast |
Map of Deauville |
Martialが主催しているウェブ・サイトとCD-ROMのイントロ部分の撮影をするためにDeauvilleを訪れました。これらはTRIを用いて5
Frenchのガイディング・カテーテルを使うことに焦点を当てたものです。EuroPCRでMartialに会った時に彼から強く誘われました。午前10時にホテルのフロントで待ち合わせました。そして、Centre
International Deauvilleという会場に行きました。そこは、ホテルから歩いて3分の距離にあり、有名なAmerican
Film Festivalが秋に開催される場所です。収録は30分で終了しましたので、同じ会場で開かれていた心不全のシンポジウムを覗きました。講演スライドは分かるのですが、討議はフランス語なので全く理解できません。30分はそこで聞いていたのですが、一人でぶらつくことにしました。
Deauvilleはノルマンディー海岸にある美しい町です。
Gucci |
Polo-Ralph-Lauren |
Longshamp |
Hermes |
Dior |
Ferragamo |
パリ在住のフランス人にとってはとても有名なリゾート地で、有名ブティックもたくさんあります。昨年ここを訪れたことがあるので、この辺りは良く知っていました。ホテル・ノルマンディーやホテル・メリーはこのDeauvilleでの典型的な建造物です。
Hotel Normandie |
Hotel Mairie |
隣町のTrouvilleまで歩きました。この2つの町は川で隔てられています。Trouvilleも綺麗な町です。もともとはリゾートではなく、漁村でした。ですから、ドックもあります。しかしながら、隣町のDeauvilleがリゾートとして有名になったため、今では多くの観光客が来ます。カジノもあります。Villeホテルは建物の高さがあるので町中でとても目立ちます。また、たくさんの小さな海鮮レストランがあります。DeauvilleとTrouvilleの間を行き来するためには橋を渡らねばなりません。
The Rive |
Map of Trouville |
Shipyard |
Casino Trouville |
Hotel de Ville |
Street in Trouville |
End of Deauville |
End of Trouville |
La Marine |
Marche de Poisson |
Fishes |
Moules Mariniere |
歩き回っている間に、日本人には会いませんでしたが、韓国の家族連れにはたくさん会いました。日本人がいなかった理由として、日本人は何時も家族旅行でなく、団体旅行するからかな、と思いました。韓国の人たちは日本人よりももっと自由に行動します。でも、この理由というのが間違いであることが後で分かりました。既に昼になっていましたし、お腹も空いたので、レストランに入りました。そのレストランの名前は“La
Marine”といい、魚市場の“Marche de Poisson”の前にあります。魚市場にはたくさんの魚があります。私は通りの席に座りました。きっと、スーツにネクタイの東洋人が一人で座っているのを見て皆、変に思ったことでしょう。私のフランスでの大好物、ムール貝のワイン蒸し“Moules
Mariniere”、魚スープそして手長えびを注文しました。
Sopes de Poissons |
Langoustines Mayonnaise |
Les Moules de Bouchot |
Menu |
この地域のムール貝はとても有名です。海岸で養殖されていて、それはBouchotと呼ばれます。シャブリの一番ハーフ・ボトルと併せてしめて65ユーロぐらいでした。味はとても素晴らしいですので、Trouvilleにお越しの際には、この小さなレストランで食事されることをお薦めします。食事が来るのを待っていると、東洋人の男の人たちが入ってきました。彼らはテレビ局の人たちでした。一人がテレビ・カメラを担いでいました。驚くべきことに、そのカメラにはKBS(韓国放送)というシールが貼ってありました。それで分かったのです。韓国の旅行番組で、この地域のことが放映されているのです。ですからたくさんの韓国人の旅行客がいるのです。
昼ごはんを終えた後、Deauvilleに歩いて戻りました。その途中のブラッセリーで「ナウシカ」の看板を見て、とても驚きました。でも、すぐにそれは「ノーティカ」であることに気づきました。Royal
Barriereホテルに戻る途中には駅がありました。その駅の名前は、仲良く「Trouville-Deauville駅」というものでした。
Brasserie NAUTICA |
Trouville-Deaville Station |
Taxi |
La Saine |
Hamon先生にさよなら、を言ってからパリにタクシーで戻りました。セーヌ川沿いにパリを横切りました。とても美しい川です。一人の女性が水上スキーをしていました。午後5時頃にシャルル・ド・ゴール空港に到着しました。そして、全日空便に乗り、日曜日6月27日に日本に戻りました。
何れにしましても、今回の旅は私にとって、一人でヨーロッパの人たちの中に飛び込んだ初めての経験でした。皆とても親切で友達付き合いしてくれて感激しました。とても感謝しています。また、この7年か8年で初めて丸3日間もインターネットと接続しませんでした。
フランス一口知識
Gasoline Price |
フランスではガソリンが日本よりも高く、1リッターが日本円にして140円ぐらいします。DeauvilleではBarrierという名前をとても良く目にしますが、これはホテル・グループの”Lucien
Barriere”のことです。Deauvilleにカジノと、ホテル二つを有しています。
|