Visiting France VIIShigeru Saito, MD, FACC, FSCAI, FJCC
|
|
|
|
|
|
|




February 27th Friday 2009
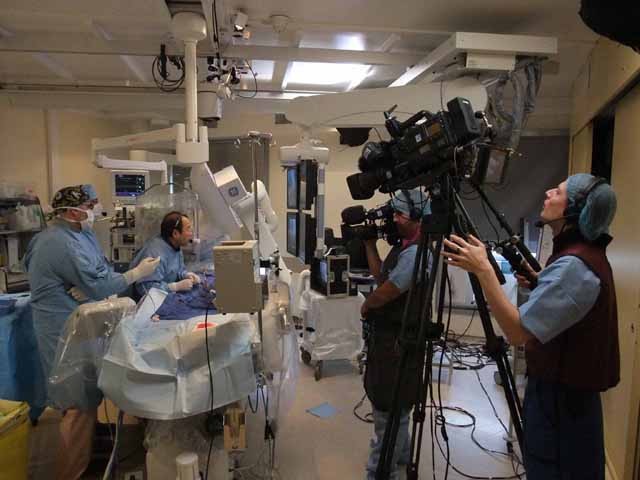
I was invited from the 2nd European CTO Workshop (Massy CTO course) as an invited operator and lecturer. Massy is a satellite city of Paris and located at the south. There is the Paris South Cardiovascular Institute, where such famous doctors as Dr. Marie-Claude Morice, Dr. Thierry Lefevre, Dr. Yves Louvard and Dr. Bernard Chevalier are working. Dr. Carlo DiMario and Dr. Hildick ?Smith from UK, Dr. George Sianos from Greece, Dr. Niklaus Reifart from Germany, Dr. Fina Mauri from Spain and other doctors famous for CTO angioplasty were also invited as faculty. The total number of attendants was almost 50. The live cases were transmitted from the hospital to a small theater called “Massy Opera”.
Since the meeting started from 1:30 PM, I had Ramen noodle in “Hokkaido” near the National Opera Theater in Paris. There were only lectures and case presentations on Friday. It was 30 minutes’ distance by car to Massy from my hotel. After finishing my roles, I came back to Paris. Because of the traffic jam, it took more than 1 hour from Massy to Paris. I had Japanese dinner at “Tagawa”. Because of the jet lag, I lost my consciousness while eating.
|
|
|
|



February 28th Saturday 2009
I woke up at 5:00 AM. After concentrating my spirit, I left the hotel at 7:00 AM and moved to the hospital. Dr. Louvard introduced me 2 cases. Both patients had previous bypass surgery almost 20 years ago. They had good LIMA-LAD graft, but their left main trunks and saphenous vein grafts were completely occluded. They showed the significant ischemia in the territory of the left circumflex artery. All of the arteries were heavily calcified. They were really difficult cases.
|
|
|
|


Dr. Sianos treated the CTO in the RCA. During the live transmission from Thoraxcenter Rotterdam to EuroPCR 2006 meeting in Paris in 2006, he was assisting me while I was treating the CTO lesion in RCA by using the retrograde approach through the septal route from LAD. After that case, he also started the retrograde approach.
I and Dr. Sianos started our own cases in 2 catheter laboratories. He took the retrograde approach through the LCX epicardial route. I started from the retrograde approach through LIMA-LAD graft. I cut a 6-French IMA guiding catheter to shorten the total length and connected again by using a 5-French introducer. The LAD was terribly calcified. I could cross a Fielder-FC guidewire from LIMA, LAD to LCX. The junction between LAD and LCX had 99% narrowing with severe angulation. It was really lucky for me to cross the wire from LAD to LCX. However, Legend 1.5 x 15mm balloon could not cross. I took an Apex-Flex 1.5 x 8 mm balloon, which crossed the lesion. I inflated the junction and LAD by 16 atmospheres. Even after these high-pressure dilatations, it was difficult to introduce a 2.0 mm balloon. While leaving the guidewire in the LCX, I exchanged the guiding catheter to a 5-French Cordis LBT LIMA catheter. By using this catheter, I could achieve a very deep engagement. The tip of the catheter reached the anastomosis between LIMA and LAD. Finally, I could place 2 DES in LAD. The final result was excellent.
After finishing my 1st case, I moved to the Massy Opera to deliver a talk. While I was doing my case, a terrible complication occurred in the other catheter laboratory. I did not know exactly what happened. Anyway, the Corsair (= Channel Dilator) inserted retrogradely was connected with a 2.0 mm balloon inserted antegradely within the patient’s RCA. Dr. Sianos spent more than 2 hours to disconnect them and failed. The patient was finally sent to the surgery. Patients’ family members were crying outside the laboratory.
|
|
|
|


After giving a talk, I returned to the hospital to treat my 2nd case. However, I could not start my case, since Dr. DiMario took long time to open the RCA due to another terrible complication. My 2nd case was terrible. The patient had a previous BMS implantation in LMT-LCX. The LIMA to LAD graft was patent. He showed a long calcified total occlusion from LMT to distal LCX. I was asked to open this long occlusion. I could cross the occlusion within the previous stent by using a Fielder-FC guidewire. After that, I took a Conquest-Pro guidewire. The lesion was really hard. I changed my mind to aim at the big OM branch. At the end of the procedure, I could achieve weak antegrade flow to this OM branch. Because I thought that I might have complications, if I continued, I quit the procedure. I did nothing harmful but something little good to the patient.
Since I was really tired for the struggling with the difficult 2 cases and sleepy, I cancelled the dinner at a very good French restaurant with doctors in the hospital. I returned to Paris and had dinner in the Japanese noodle restaurant “HIGUMA”. I went to my bed before 9:00 PM.
March 1st Sunday 2009
I left the hotel for CDG International Airport to catch the AF 0006 flight departing at 13:15 for New York. Next my visit to Paris will be during EuroPCR 2009. I will do live transmission from Massy on TRI.
フランス訪問記 - VII
湘南鎌倉総合病院 心臓センター循環器科
齋藤 滋
数年ぶりのパリ訪問
2009年2月26日木曜日11:55 AM発のNH 205便で成田を発ち、パリに向かいました。 11時間半の飛行の後、シャルル・ド・ゴール(CDG)空港に到着しました。飛行機の中では一 睡もせずに映画を見ていました。パリにはもう何回も来ていますが、今回は数年ぶりです。 宿はエッフェル塔近くのPullmanホテルでした。夕食は「オンワード樫山」が経営してい る「円」という蕎麦屋で頂きましたが、ものすごく値段が高く、しかも味はニューヨークの 「そば こう」よりかなり落ちます。
|
|
|
|
|
|
2009年2月27日金曜日
今回私は第二回ヨーロッパ慢性完全閉塞ワークショップ(Massy CTO course)に術者およ び演者として招聘されました。Massyはパリの南に位置する衛星都市です。そこにはパリ南 心臓病センターがあり、有名なMorice先生、Lefevre先生、Louvard先生そしてChevalier 先生が働いておられます。私の他にもイギリスからDiMario先生、Hildick-Smith先生、ギ リシャのSianos先生、ドイツのReifart先生、スペインのFina先生などCTOでは有名な先 生方も呼ばれました。会の参会者は50名ぐらいでした。ライブは病院からMassy Operaと 呼ばれる小さな劇場に中継されました。
会はこの日の1:30 PMから始まりましたので、昼食はパリ・オペラ座近くの「北海道」 というラーメン屋さんで食べました。この日は講演や症例報告だけでした。ホテルから Massyまでは車で30分ぐらいでした。講演を終えてパリに戻ったのですが、交通渋滞のた め1時間以上もかかりました。夕食は「田川」という和食の店でとりましたが、時差ボケで 食べている途中で意識消失発作が起こりました。
|
|
|
|
2009年2月28日土曜日
5:00 AMに起床し、精神集中を行い、7:00 AMにホテルを出て病院に向かいました。 Louvard先生に僕の症例2症例を見せて頂きました。両方とも20年ぐらい前に冠動脈バイ パス手術を受けておられ、良好なLIMA-LADグラフトがありましたが、左主幹部と静脈グ ラフトは閉塞し、回旋枝領域に広範な虚血を呈している症例です。動脈は全部激しい石灰化 を呈していました。本当に難しい症例でした。
|
|
|
|
Sianos先生は右冠動脈の慢性完全閉塞を治療しました。彼は、私が2006年にパリで開 催されたEuroPCRの最中に、ロッテルダムのThoraxcenterで私が逆行性アプローチで治療 し、ライブ中継した右冠動脈の慢性完全閉塞症例で、私の助手をしてくれました。それを見 て、逆行性アプローチを彼も開始したのです。
私とSianos先生はそれぞれのカテ室で開始しました。彼は回旋枝からの逆行性アプロー チをしました。私は、LIMA-LADグラフト経由の逆行性アプローチをしました。カテの長さ を短くするために、6FrのIMAガイディング・カテーテルを切断し、5Frのシースで繋ぎま した。左冠動脈前下行枝はひどい石灰化でした。LIMA, LADを介して、LCXにFielder-FC を通過することができました。LADと回旋枝の接合部には99%狭窄があり、しかもひどく 屈曲していたのです。ワイヤーをクロスできて本当にラッキーでした。でも、この後、1.5 x 15 mmのLegendバルーンは通過できませんでした。Apex-Flex 1.5 x 8mmバルーンが通過 し、それで16気圧でLADも拡張しました。この高圧拡張の後でも2.0mmバルーンを持っ ていくことは大変でした。ガイドワイヤーを回旋枝に残しながら、ガイディング・カテーテ ルを5Fr Cordis LBT LIMAカテーテルに交換しました。このカテのお蔭で、LIMA-LAD吻 合部の辺りまで持ち込むことができました。結局薬剤溶出性ステントを二つ左冠動脈前下行 枝に植え込みました。結果はすばらしいものでした。
一例目を終えて、講演をするためにMassy Operaに戻りました。私が自分の症例を治療 している間に、他のカテ室では恐ろしい合併症がおこっていました。何が起きたのかは正確 には知りません。しかし、どちらにしても、逆行性に挿入されたCorsair (=Channel Dilator) と、順行性に挿入された2.0mmバルーンが患者さんの右冠動脈の中で接合してしまったの です。Sianos先生は何とかしようと2時間以上粘りましたが、うまくいきませんでした。結 局患者さんは手術に送られました。患者さんのご家族はカテ室の外で泣いておられました。
|
|
|
|
講演を終えてから病院に戻り、二症例目にとりかかろうとしました。しかし、すぐに開 始できなかったのです。何故って、僕の前にやっていたこれもまた信じられない合併所のた め、DiMario先生が右冠動脈を開通させるのに、とても時間がかかっていたのです。僕の二 例目はひどい症例でした。患者さんは左主幹部から左冠動脈回旋枝にかけてBMSを以前植 えられていました。LIMA-LADは開通しているのですが、左主幹部から左冠動脈回旋枝遠位 がひどい石灰化を伴う慢性完全閉塞となっていました。ステント内の閉塞部分は何とか Fielder-FCでクロスできたのですが、その後はとても硬く、Conquest-Proを用いました。 病変は本当にとても硬かったのです。このため方針を変更し、大きなOM枝に向けて再開通 を図ることにしました。手技の最後には何とか弱いながらも順行性の血流をこのOMにもた らすことができました。これ以上続ければきっと合併症を起こしかねない、と考え、そこで 手技を終えました。私は患者さんに対して何も悪い事はしていませんし、少し良いことをし ました。
困難な二症例の治療にとても疲れてしまいましたし、また眠くもありました。このため、 最上級のフランス料理レストランで予定されていた、この病院の先生方との夕食はキャンセ ルして、パリに戻りました。そして、ラーメンの「ヒグマ」で夕食を摂りました。9:00 PM にはもう寝ていました。
2009寝年3月1日日曜日
13:15発のニューヨーク行きAF 0006便に乗るためにホテルを出てCDG空港に向かいま した。今度パリを訪れるのはEuroPCR 2009の時です。この時、再びMassyからEuroPCR 会場にTRIのライブ中継を行います。