Introduction
I came back to Moscow again after my visit in April this year [LINK]. My 1st visit at Moscow was 2 years ago on June 5, 2002, when I was invited directly by e-mail from Professor Alekyan as one of the invited foreign faculty members in the congress of the 3rd International Moscow’s Course on Endovascular Surgery of Congenital and Acquired Heart Defects, Coronary and Vascular Pathology. The other faculty members included Professors Jean Marco and Yves Louvard from France, Professor Antonio Colombo from Italy, Professor Josef Ludwig from Germany, Professor U. Sigwart from Switzerland, and other world-famous doctors. I did 2 lectures and 3 live cases there. During my live case transmission, I had a chance to use Cypher stent in 1 patient. That was my 1st experience to use Cypher stent. This time, the congress was the 5th one.

Midnight Sun |

Cafe Pushkin |

Night Street |

President Hote |
As I introduced in the “Visiting Moscow ? II [LINK], only 2 airline
companies have direct flight between Moscow and Tokyo. One is Russian National Airline Company, Aeroflot, and another is Japan Airline (JAL).
Because JAL has only 1 flight every week on Tuesday from Tokyo, I took a NH1209 flight (ANA) to Frankfurt on June 07 Monday, 2004,
which is connecting with a LH3188 flight (Lufthansa) from Frankfurt to Moscow. The NH1209 flight departed from the Narita airport
around 12:15 with the delay of 40 minutes. The departure of the LH3199 flight from Frankfurt was again delayed due to a small accident.
According to the in-flight announcement, another Lufthansa airplane staying at the Moscow airport had some machine trouble and needed
several airplane parts transferred from Frankfurt. Our flight had to send these parts to Moscow and waited for them. After 3 hours’ flight,
we finally arrived at the Moscow airport later than 11:30 pm of June 7, when the sky was not dark due to the midnight
sun. After checking in the President Hotel, I went to Cafe Pushkin, where we can have high-class traditional
Russian foods 24 hours a day;.
NHK News |
After having black caviar, Borshch soup and Beef Storganov, I came back to the hotel later than 1:00 AM of next day. Even in
the late night, we can see many beautiful and brightened signboards along the streets;. Because June is
the best season to visit Moscow, all of the hotels were fully booked. Since this time I could not book my favorite hotel, Hotel
Baltschug Kempinski Moscow, where we can use high-speed Internet connection any time, I stayed at this Soviet Union style hotel.
The outside of President Hotel is somehow overbearing. In this hotel, I had the difficulty in connecting
my computer to Internet. They provided me the combination of local call number of “3555”, account name and password for
the modem-line connection. However, even after the connection was established at the speed of less than 52 Kbps, I often could not
retrieve or send e-mails nor browse home pages. It was lucky for me to be able to watch the international program of NHK
TV;.
June 08 Tuesday, 2004
Plate in the Auditorium |

Bakoulev Center |

Auditorium
|

Dr Anton showing cases |
Program |

Attendants |

My Presentation
|

9th Floor of the Hospital |
The congress was held in the Bakoulev Scientific Center for Cardiovascular Surgery. This hospital is the Government Cardiovascular
Center which is run by Ministry of Health of the Russian Federation and Russian Academy of Medical Sciences (RAMS). The hospital was
moved to this place, where is just at the border of Moscow city, on October 9, 1998 from the downtown area of Moscow;. The hospital building
is huge ;. This time, we had those famous international doctors as
Dr. Louvard, Dr. Ludwig, Dr. Sigwart and Dr. Gary Mintz as International Guest Faculty. The organizing committee assigned me 1 lecture
and 2 live cases this year. The title of the lecture that they asked me was again “PCI for Chronic Total Occlusion”. During the last 2 years,
I made lectures about CTO. By looking back at the previous my presentations, I can know that my knowledge and skills of PCI for CTO lesions
have progressed a lot during these 2 years. Since my lecture was scheduled from 9:30 AM, I arrived at the big auditorium of Bakoulev Scientific
Center for cardiovascular surgery at 9:00 AM;. When I arrived there, Dr. Staferov Anton showed me my cases by
using his Toshiba laptop computer;. They showed 2 cases with CTO lesions. I accepted their case
selection for me. Dr. Anton can speak fluent English. I asked him, “Why can you speak so fluent English? Have you studied in foreign countries?”
His answer was “No, I cannot speak fluent English. I studied only in Russia. I studied Interventional Cardiology here in Bakoulev Center
under Professor Alekyan.” Also, he added “Case selection for you is always quite easy, because you can do all cases.”
I know that actual congress proceedings always tend to be behind the schedule;. My lecture was started
from 10:10 AM. Many people were in the auditorium;. My presentation invoked a lot of concerns from the audience.
I had many questions;. I modified the presentation a little bit, which I used during the last EuroPCR
live transmission [LINK], for this lecture
in the airplane. I added a case, whom I did the retrograde guidewire insertion through the collateral channel.
After finishing my lecture, I hurried up to the 9th floor of the hospital, where they have 6 catheter laboratories.
. This time, I used the room equipped with Philips machine (Integris BH-3000). T
he machine is a biplane machine, but the lateral projection system did not work. Thus, the machine was actually a single plane machine.
Case1-LCX pre
|

Doing Case1-1 |

Doing Case1-2
|

Professor Alekyan |

Case1-LAD final |

Case1-LCX final |

Memorial Photo with Case1 |

Cafeteria |
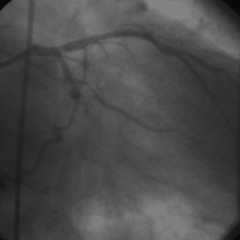
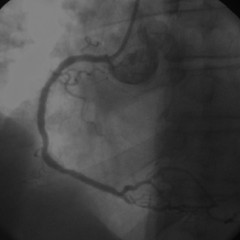
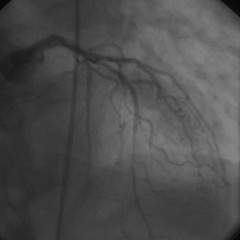
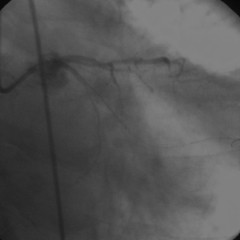
My 1st live case started from 11:10 AM. The 1st case was a 61-years old gentleman with triple vessel disease and previous
anterior myocardial infarction. His left ventricular function was good. The RCA lesions were distal. He had a 3-years CTO lesion
in the proximal LAD and another occlusion in the proximal LCX;. My approach for this patient was
transfemoral approach using a 7 French guiding catheter with the aid of simultaneous contra-lateral RCA angiography using
a 5 French diagnostic catheter. I had difficulties to engage guiding catheters into LCA. After several trials of guiding catheters,
an XB 3.0 guiding catheter was finally successful. First, I used a Magic-FA guidewire with a Transit microcatheter to the CTO in LAD.
The lesion was unexpectedly hard, although I could not see any remarkable calcification. Because the Magic-FA guidewire could not
make even a tiny entry into the occlusion, I changed it to Conquest-Pro. The guidewire gradually advanced into the occlusion and
finally went into the false lumen;. Then, I took a Magic-EX guidewire to perform the double guidewire technique.
However, the proximal cap of the occlusion was so hard that I could not make any entry by using this guidewire. I had to decide whether
I should do the double guidewire technique by using 2 Conquest-Pro guidewires or do something else. I thought that, if I took another
Conquest-Pro guidewire, I created another entry to the false channel. Thus, I decided to take out the Magic-EX guidewire, to replace
the initial Conquest-Pro guidewire by it, and to abandon the double guidewire technique. Because the hard proximal cap had already
a small hole created by the previous Conquest-Pro guidewire, the Magic-EX guidewire gradually went into the occlusion. The guidewire
now entered into the distal true lumen;. I am very sorry that I cannot show these processes by photos,
since I received only last half parts of CD for this case. I am now asking Dr. Anton to send me the initial half of CD. I crossed the lesion
with a Magic-FA guidewire, and waited for the transmission start. After Dr. Louvard finished his case with the left main bifurcation lesion,
the transmission came to us. Before my case, Professor Alekyan came to our catheter laboratory and received a TV interview by
Russian National Broadcasting Compan;.
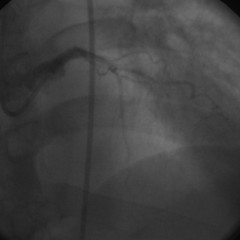
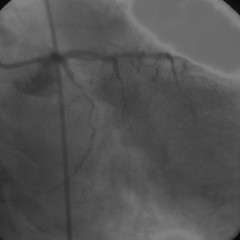
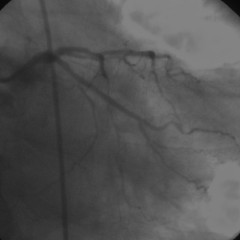
As I expected, a 1.5 mm balloon (Stormer,Medtronic) could not pass the lesion. I showed the “Anchor Balloon” technique by inflating
a 2.5 mm balloon in the diagonal branch proximal to the occlusion. The 1.5 mm balloon successfully advanced into the occlusion. I placed
one 3.0 x 33 mm Cypher stent there;. I could hear that this success drew enthusiastic applause from
the audience. Next, I attacked the proximal occlusion of LCX. I used the previous Magic-FA guidewire and easily passed the lesion.
I placed one 2.75 x 33 mm Cypher stent there;. Everybody in the laboratory including the patient was
quite happy with the results. I asked the patient to take a memorial photo together with Dr. Anton;.
I had lunch in the cafeteria within the hospital;. There is a food shop in the cafeteria, where I bought an ice candy.
The price was 10 rubles, which is almost equivalent to 40 Japanese yens.

Case2-RCA pre |

Doing Case2-1 |
Case2-RCA final
|
Case2-LAD pre |

Doing Case2-2 |
Case2-LAD passed |
Case2-LAD kissing |
Case2-LAD final |
Case2-LCX pre |
Case2-LCX passed |
Case2-LCX Anchor |
Case2-LCX Tornus |
Case2-LCX final |

Memorial Photo with Case2 |

Road over the Hill |

Cathedral of Christ the Saviour |

Russian Army Troop |

Gate |
| |
|
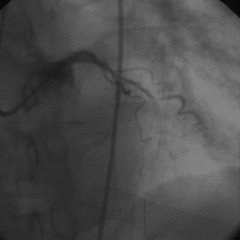
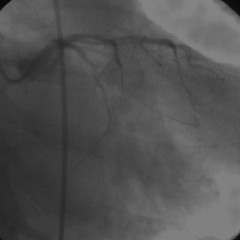
My 2nd case started around 4:00 PM. This case was a 66-years old gentleman with triple vessel disease. His LAD and LCX were
occluded at least before 3 or 5 years ago. Because of unstable angina, he received a bare metal stent implantation in the proximal RCA
in November 2003. His symptoms recurred recently. Coronary angiogram showed an in-stent restenosis within a 3.0 x 15 mm Be2Stent
in the proximal RCA;. I again took the right femoral approach;. For this patient,
I did not do simultaneous bilateral coronary angiographies and took a 6 French guiding catheter, since his left main coronary artery looked
small in diameter. First, I placed a 3.5 x 28 mm Cypher stent in the proximal RCA;. Then, I took a Magic-FA
guidewire again to cross the CTO lesion in the middle of LAD just distal to the 1st diagonal branch;.
The guidewire initially went into the false lumen. I though it would be very difficult to do a double guidewire technique in this
small LAD;. Thus, I tried to put the guidewire into the distal lumen. I was lucky to be successful to
achieve the distal true lumen by this guidewire;. After sequential kissing balloon dilatations;,
I placed one 2.25 x 33 mm Cypher stent there;. Again, I heard loud handclapping sound
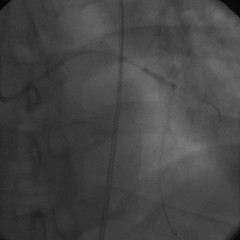
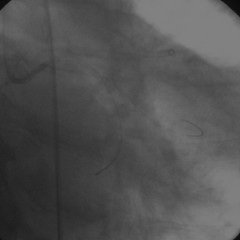
by the audience. The proximal LCX also showed a CTO;. I took the same Magic-FA guidewire together with a
Transit microcatheter. The artery showed a bent at the occlusion. After forceful pushing, the guidewire passed through into the distal true
lumen;. Again I could not cross the lesion by a 1.5 mm balloon (Stormer). I tried to do the “Anchor Balloon”
technique;, but I could not 2 Stormer balloons simultaneously into this 6 French guiding catheter (Launcher,
Medtronic). They did not have any thin-shaft balloons like Maverick from Boston-Scientific Company. I took Tornus penetrating system
from my bag and used it. Tornus went through the occlusion;. Again, everybody in the auditorium became
enthusiastic. Finally, I placed a 3.0 x 33 mm Cypher stent there. The final angiogram was so surprised that Professor Alekyan and other
faculty members told me “It’s a magic.”; I took a memorial photo together with the patient and
Dr. Anton. Thus, my live case transmission for 2 patients and 3 CTO lesions were finished
with a great success and big applause. It was already 5:10 PM.
After these cases, I returned to the hotel. On the way to the hotel, we passed through the hill, over where any foreign army troops
could not pass into the city of Moscow;. General Napoleon as well as German Nazis troops returned
from this hill. From the top of this hill, people use to see beautifully brightened golden roofs of Russian Orthodox Church. Many of
them were destroyed during the era of the Communistic Party. One of them was re-built about 10 years ago;.
The place used to be a swimming pool before the Church was re-built.There are several monuments to memorize
these histories on the road. One of them is the stature of Russian army troop;, and another is the
gate;. Near the hotel, I could see a tall building of the University of Moscow, which is the highest-rank university
in whole Russia;.

University of Moscow |

Georgian Restaurant |

Godunov Outside |

Godunov Plate |

Beef Storganov |

Gipsy Music 1 |

Gipsy Music 2 |

Moscow Airport |
I spent almost 1 hour in a Georgian Restaurant, where Professor Alekyan booked to hold a Dinner party from 7:30 PM.
All of the faculty members came to me and gave me the highest applause. Many of them expressed the warm proposal
to invite me to their own countries to learn the PCI techniques for CTO lesions. After saying “Good Bye” to them, I hurried to one of
my favorite restaurants in Moscow, “Godunov”;, where we can enjoy delicious Russian cuisines and
Russian or Gipsy folk live music. I cannot know from the plate of the restaurant that it is “Godunov”;.
Beef Storganov of this restaurant is delicious;. I could enjoy the live music by a Gipsy family;.
June 09 Wednesday, 2004
Before I took the return flight to Japan by LH3185 to Frankfurt and NH210 from Frankfurt to Tokyo, I had free time to be relaxed.
Moscow International Airport looks belonging to the old communistic days;. They said that they had 10,000
stents implantation in 6,000 PCI cases a year in whole Russia. Those cases are done by 50 to 60 hospitals. This hospital number is
quite different from that informed to me last year [LINK].
It was 10,000 hospitals to do angioplasty procedures. I guess that both hospital numbers of 50 to 60 and 1,000 are not correct.
In Bakoulev Center, Dr. Anton told me they had almost 300 PCI cases last year. This case number should be the biggest one in whole Russia.
Thus, I guess that the average number of PCI cases in each hospital shall be less than 100 a year. From this calculation, I can guess
that almost 100 hospitals in Russia are doing PCI procedures. Anyway, I can tell that the PCI procedures have been centralized to main
hospitals during the past several years in Russia.
Hints in Russia
Moscow is the city of very rapidly growing. The population in Moscow is now more than 20 million. Among them, more than 8 million
people are without any formal registration. Many people come to Moscow to find jobs especially from Vietnam or Arabian countries.
The price of gasoline is not expensive in Russia. It is about 40 Japanese Yen for 1 litter of normal gasoline.
We have to know about those Russian words: “Spasiba” and “KharaSHO” for “Thank you” and “Very nice”.
モスクワ訪問記III
湘南鎌倉総合病院 心臓センター循環器科
齋藤 滋
はじめに
今年4月にモスクワを訪問した後、再び今回モスクワを訪れました[LINK]。私が初めてモスクワを訪れたのは2年前の2002年6月5日のことでした。その時、私はAlekyan教授から直接電子メールを受け取り、第三回モスクワ国際血管内手術学会に外国招聘講師としての参加を要請されました。この時の他の有名な外国招聘講師としては、フランスからMarco先生とLouvard先生、イタリアからColombo先生、ドイツからLudwig先生、スイスからSigwart先生などが参加されました。この時、私は講演二つと三例のライブデモンストレーションを行いました。そして、このライブデモンストレーションの時に私にとって初めての経験であるCypherステント植え込みを行いました。今回の学会は第五回の学会でした。
Midnight Sun |
Cafe Pushkin |
Night Street |
President Hote |
モスクワ訪問記II[LINK]で紹介しましたように、
モスクワ-東京間には2社しか直行便が飛んでいません。その内の一つはアエロフロートであり、もう一つは日本航空ですが、
日本航空直行便は週一便火曜日のみですので、私はフランクフルト行きの全日空NH1209便に2004年6月7日月曜日に乗りました。
この便はフランクフルトでモスクワ行きのルフトハンザLH3188便に接続しています。全日空便は40分遅れの12:15に成田を飛び立ちました。
フランクフルトからのLH3188便もある理由で遅れました。何でも他のルフトハンザ便がモスクワ空港で故障していまい、
その便のために部品を持ち込む必要があり、その部品の収容のために遅れたということです。
3時間の飛行の後で6月7日午後11時30分過ぎにモスクワ空港に着きました。しかし空は白夜のためにまだ薄らいでいました。
プレジデント・ホテルにチェック・インしてからCafe Pushkinに行きました。
NHK News |
そこでキャビア、ボルシチそしてビーフ・ストルガノフを食べてから部屋に戻りましたが、時刻はもう午前1時になっていました。
こんな夜遅くでも街中には明るい綺麗なネオンがありました。6月というのはモスクワにとって最も良い季節です。このため、
市内のホテルは満員でした。ですから私の定宿であり、高速インターネット接続可能なケビンスキー・ホテルも一杯で
仕方なくこの旧ソビエト様式のホテルに泊まることになりました。このホテルの外観は何というか威圧的なものがあります。
しかしながら、インターネット接続には難儀しました。ホテルの言う通りに3555という番号にダイアルし、彼らの言う接続名と
パスワードを入力すれば52Kbpsで接続できました。しかし、それでもなかなか電子メール送受信は出来ませんし、
ホームページ閲覧も困難でした。でも、室内テレビではNHK国際放送ニュースを見ることが出来ました。
2004年6月08日火曜日
Plate in the Auditorium |
Bakoulev Center |
Auditorium
|
Dr Anton showing cases |
Program |
Attendants |
My Presentation
|
9th Floor of the Hospital |
学会はバクロフ心臓センターで開催されました。この病院はロシア保健省に所属し、ロシア医学アカデミー(RAMS)によって運営されている
国立心臓センターです。実はこの病院は1998年10月9日にモスクワ中心部からこのモスクワ市外れに移転したのです。病院の建物はとても巨大です。
今回の主だった招聘外国人講演者は、Louvard先生、Ludwig先生、Sigwart先生そしてMintz先生でした。今回学会組織委員会は私に、
講演一つと二例のライブデモンストレーションを依頼しました。彼らから依頼された講演は「慢性完全閉塞病変に対する経皮的冠動脈インターベンション」でした。
この2年間私は同じタイトルで講演をしてきました。これらの講演スライドを振り返って見ましたが、この2年間で私の慢性完全閉塞に対する
知識や技術が進歩してきたことが分かりました。
私の講演は午前9時30分から予定されていましたので、私はバクロフ病院大講堂に午前9時に行きました。そこではAnton先生が待っていて、
彼の東芝ラップトップコンピューターを用いて私に症例を見せてくれました。彼らが私に用意したのは慢性完全閉塞の2例でした。私はこれらの2例に
対してPCIを行うことを承諾しました。彼は流暢に英語を喋ります。彼に、「どうしてそんなに英語がうまいの? 外国に留学したことあるの?」と、聞きました。
彼は、「自分の英語はそんなにうまくない。自分は外国に留学したことない。自分はこのバクレフ病院でAlekyan教授からPCIを習っただけだ。」と、答えました。
また、彼は、「齋藤先生へのライブデモンストレーション症例を選ぶのは簡単だ。何故って、齋藤先生はどんな症例でもやれるから。」と、付け加えました。
大体いつも学会進行はスケジュールから遅れます。私の講演は午前10時10分に始まりました。会場にはたくさんの人々がいました。私の講演は
皆の関心を呼び、多くの質問を受けました。今回私は先のEuroPCRライブデモンストレーション
[LINK]で用いたスライドを飛行機の中で修正して
用いました。特に、副血行路を通して逆行性にガイドワイヤーを通過させる方法を追加しました。
講演を終了して、9階にあるカテ室に急ぎました。この病院には6部屋のカテ室があります。今回、私はPhilips社製BH-3000があるカテ室を用いました。
本来このマシンはバイ・プレーンですが、側面透視は壊れていて、現実にはシングル・プレーンしか用いることは出来ませんでした。
Case1-LCX pre
|
Doing Case1-1 |
Doing Case1-2
|
Professor Alekyan |
Case1-LAD final |
Case1-LCX final |
Memorial Photo with Case1 |
Cafeteria |
私の第一症例は午前11時10分にスタートしました。61歳男性で、前壁梗塞を有する3枝病変の患者さんでした。左室機能は良好でした。
右冠動脈病変は末梢のものでした。左前下行枝近位部の慢性完全閉塞病変は3年経過したものであり、これとは別に左回旋枝近位部にも
閉塞病変がありました。7Frのガイディング・カテーテルを用いて経大腿動脈的冠動脈インターベンションにより5Fr造影用カテーテルを用いた
対側造影を併用することにしました。左冠動脈にガイディング・カテーテルを挿入するのは困難で、何種類かのガイディング・カテーテルを試してから
最終的にXB 3.0によりうまくいきました。まずTransit + Magic-FAにより開始しました。石灰化も見られないのに、予想に反してこの閉塞病変は非常に
硬いものでした。Magic-FAではどうしても閉塞部の中に入ることができませんでしたので、Conquest-Proに交換しました。このガイドワイヤーは
閉塞部の中に突き刺さりましたが、そのまま偽腔に入ってしまいました。そこで、Magic-EXを用いてDouble Guidewire Techniqueを試みましたが、
閉塞近位端が非常に硬いため、Magic-EXは全く閉塞部の中に入りませんでした。そこで、もう一本Conquest-Proを取り出してあくまでも
Double Guidewire Techniqueを行うか、あるいはそうしないかを考えました。もしももう一本Conquest-Proを用いても再び偽腔に入るだけだろう、
と考えました。そこで、Double Guidewire Technique を止めて、Magic-Exを一旦抜いて、既に挿入されていたConquest-Proに置き換えました。
既に閉塞部の硬い近位端はConquest-Proによって小さな穴が開いているので、Magic-EXは閉塞部の中に入っていきました。そして、ついに真腔を
捉えることができました。私が受け取ったCDの中にはこの部分が収録されていませんでしたので残念ながら写真をお見せすることはできません。
今、Anton先生に送って欲しい、と言っているところです。このMagic-EXで病変を通過した後、私は中継を待ちました。Louvard先生による
左主幹部分岐部病変に対するステント植え込みが終了した後、Alekyan教授がカテ室に来られました。彼はロシア国営テレビのインタビューに応えられました。
私が予想していたように、1.5 mm Stormerバルーンでは病変をクロスすることが出来ませんでした。そこで、2.5 mmバルーンを対角枝で拡張して、
アンカー・バルーンを行いました。これによって1.5 mmバルーンは閉塞部に進み、最終的に3.0 x 33 mmのCypherステントを植え込んで終了しました。
この手技を見て聴衆から大きな拍手が沸き起こりました。次に、回旋枝近位部の閉塞にとりかかりました。先に用いたMagic-FAによって病変をクロスして、
2.75 x 33 mmのCypherステントを植え込みました。患者さんもカテ室内の皆も全てとても喜びました。そして、Anton先生と患者さんとも共に記念写真を撮りました。
病院内の食堂で昼食をとりました。食堂内には売店があり、そこで10ルーブルでアイス・キャンディーを買いました。日本円で40円ぐらいです。
Case2-RCA pre |
Doing Case2-1 |
Case2-RCA final
|
Case2-LAD pre |
Doing Case2-2 |
Case2-LAD passed |
Case2-LAD kissing |
Case2-LAD final |
Case2-LCX pre |
Case2-LCX passed |
Case2-LCX Anchor |
Case2-LCX Tornus |
Case2-LCX final |
Memorial Photo with Case2 |
Road over the Hill |
Cathedral of Christ the Saviour |
Russian Army Troop |
Gate |
| |
|
私の2例目は午後4時頃に始まりました。66歳の3枝病変の男性でした。左前下行枝も左回旋枝も3から5年ぐらい前に完全閉塞していました。
不安定狭心症となったために去年の11月に右冠動脈近位部に対してBMS植え込みがされていました。でも最近再び症状が出現し、冠動脈造影の結果、
右冠動脈に植えられた3.0 x 15 mmのBe2Stent内のステント内再狭窄を認めました。この症例でも右大腿動脈からの経大腿動脈的冠動脈インターベンション
を用いましたが、対側造影は用いませんでした。左冠動脈は非常に細かったので、6Frのガイディング・カテーテルを用いました。まず3.5 x 28 mmの
Cypherを右冠動脈近位部に植え込みました。次いで、Magic-FAを用いて第一対角枝分岐部の左前下行枝CTOに挑みました。ガイドワイヤーは最初、
偽腔に入りました。しかし、Double Guidewire Techniqueを行うには左前下行枝が細すぎると考えました。そこで、私はこのMagic-FAを真腔に
導入すべく試みました。幸にもガイドワイヤーは真腔に入りました。逐次キッシング拡張を行ってから2.25 x 33 mmのCypherを左前下行枝に植え込みました。
ここでも会場からは拍手喝采が沸き起こりました。左回旋枝もCTOでした。先に用いた同じMagic-FAによって通過を試みました。この病変はちょうど屈曲部に
存在しました。強く押すことによりガイドワイヤーは閉塞部を超えて真腔に入りました。1.5 mmのStormerバルーンでは病変通過できませんでしたので、
アンカーを試みました。しかし、Stormerバルーンではシャフトが太すぎで6Frガイディング・カテーテル内に二本同時に持ち込むことは不可能でした。
残念ながらシャフトの細いMaverickはカテ室内にありませんでした。このため、私は、自分の持ち込んだバッグ内からトルナスを取り出し、これにより病変通過に
成功しました。再び会場では拍手喝さいが沸き起こりました。最後に3.0 x 33 mmのCypherを植え込んで終了しました。最後の造影を見て、
Alekyan教授や他のFacultyの先生方は「これはマジックだ!」と、言われました。最後にAnton先生と共に患者さんと記念写真を撮りました。こうして私の2例、
3箇所のCTOに対するPCIは大成功で終わり、皆から拍手喝采を受けました。既に時刻は午後5時10分でした。
この後、私は一旦ホテルに戻りました。途中、丘を越えて行きます。この丘をこれまでいかなる外国軍隊も超えてモスクワ市内に入ることができませんでした。
ナポレオン将軍も、ナチス軍もこの丘で引き返したのです。この丘に立つと、ロシア正教教会の輝く屋根が見えたそうです。それらの教会の多くも
共産党時代に破壊されました。その中の一つは10年前に再建されました。この場所には以前はプールがあったそうです。道路にはこれらの歴史を記念する
いくつかのモニュメントがあります。その一つはロシア軍歩兵の彫像であり、あるいは記念のゲートです。ホテルの近くからは、モスクワ大学の高い建物が見えました。
この大学はロシア最高学府です。
University of Moscow |
Georgian Restaurant |
|
Godunov Outside |
Godunov Plate |
Beef Storganov |
Gipsy Music 1 |
|
Gipsy Music 2 |
Moscow Airport |
この後、午後7時30分からAlekyan教授によって主催された夕食会のためグルジア料理レストランに行き、1時間ほど費やしました。Faculty全員が
参加しましたが、皆私のところに来て、賞賛の言葉を述べられました。そして、皆が「是非、うちに来てどのようにCTOに対してPCIを行うのか実演して欲しい」と、
請われました。皆に別れを告げた後、私はモスクワで一番好きなレストラン「ゴドノフ」に行きました。ここでは最高のロシア料理だけでなく、ロシア民謡あるいは
ジプシー音楽の実演を楽しむことが出来ます。でも看板からそれが「ゴドノフ」であることを読み取ることは困難です。ビーフ・ストルガノフはとてもおいしいです。
この日はジプシー家族の生演奏を楽しむことが出来ました。
2004年6月9日水曜日
LH3185によりフランクフルト経由、NH210で日本に帰る前、少し自由な時間がありました。モスクワ国際空港は古き共産党時代の雰囲気があります。
ロシア全体では年間6,000例の冠動脈インターベンションが行われ10,000個のステントを用いられているそうです。これらの症例は全国50から60の病院で
行われているそうです。でもこの情報は、昨年私が得た情報[LINK]
である1,000の病院というものとは大きく異なります。私が思うに、50から60という数字も、1,000という数字も両方が正しくないでしょう。Anton先生によれば、
バクレフ病院では昨年300例のPCIが行われたそうです。この数字がロシア全体の中では最大のものでしょう。ですから、一つの病院当り平均で
年間100にも満たない数、というのが本当でしょう。こう考えれば、ロシア全土では100ぐらいの病院がPCIを行っていると推定されます。どちらにしても
この数年でPCIを行う施設の集約化が起こっているのでしょう。
ロシアでのヒント
モスクワは急速に発展している都市です。モスクワの人口は2千万人以上です。この中の800万人は不法滞在者です。仕事を求めて、ベトナムあるいは
アラブ諸国から多数の人々がモスクワに来ているそうです。ロシア国内のガソリンの値段は高くはありません。1リットルが日本円にして大体40円ぐらいです。
以下のロシア語ぐらいは知りましょう。「スパシーバ」と「ハラショ」です。これらはそれぞれ、「ありがとう」と「すばらしい」です。
|