Introduction
The most intimate friend of mine in India,
Dr. Tejas Patel and I have been planning to hold the live
demonstration and workshop for transradial approach in his
home town, Ahmedabad. Transradial coronary intervention
is getting more and more popular in India similarly with
the rest of the world. However, there are still many opponents
against TRI especially among the relatively aged and already
established Interventional Cardiologists. We had several
discussions and finally decided to hold the live demonstration
course in January 2005. The name of the meeting is TRICO
2005, which means “Trans Radial Intervention COurse 2005”.
I and Tejas are the course directors, and we involved Dr.
Ferdinand Kiemeneij from Netherlands and Dr. John Coppola
from USA. This time, I also invited Radialists from Japan:
Dr. Shin-ichi TOHYAMA, Dr. Yoshifumi Kan, Dr. Hideaki SAKAI,
Dr. Motomaru MASUTANI, Dr. Tetsuya HATA as well as my colleague,
Dr. Yoshio TAKETANI.
| |
|
TRICO Program
1 |
TRICO Program
2 |
We met together in NARITA International Airport
and took the JAL flight of JL723 departing at 11:45 AM for
Kuala Lumpur on January 20 Thursday, 2005. The flight arrived
at Kuala Lumpur International Airport around 6:30 PM of
Malaysian Standard Time. We supposed to transit to the Malaysian
Airline of MH178 for Ahmedabad very quickly. However, since
the departure was delayed by almost 1 and half hours, we
had to spend almost 2 hours in the transit lounge. The new
KL airport is very comfortable. I could connect my laptop
computer with Internet freely by WiFi high-speed network
there. After almost 5 hours' flight from KL, we finally
arrived at Ahmedabad International Airport around 0:00 AM
midnight of January 21 Friday, 2005. We took a coach together
to the hotel “The Pride Hotel Ahmedabad”. It was already
0:30 AM, which was 4:00 AM by Japan Standard Time. After
checking in my room, I tried to find high-speed Internet
connection but failed. I called people from the front desk.
However, it was very sorry that I could not get any high-speed
Internet connection within the hotel.
The hotel is in the center of Ahmedabad city.
I could see a very big and rich house building next to the
hotel from the window of my room.
January 21 Friday, 2005
Since there is 3 and half hours' time difference
between Japan and India, I again fell into sever jet lag.
I waked up and slept again every 1 hour. Finally, I left
the bed and completely waked up at 5:30 AM (9:00 AM in Japan
Standard Time).
After that, I did several works by using my laptop computer.
I had breakfast from 7:00 AM and left the hotel for Sterling
Hospital at 8:15 AM. They have 2 catheter laboratories:
one is equipped with a Siemens' single-plane flat panel
machine, and another with a Philips' single-plane H-5000.
The rooms were crowded by doctors, nurses, technicians and
TV staffs. Everybody looked be in high tension.
| |
|
|
Sterling Hospital |
Everybody in
Labo? |
TV Settings |
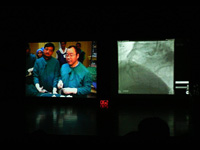
Although the meeting was scheduled to start
from 8:45 AM with Welcome Address by Tejas, since the starting
of the meeting was delayed and we had a lecture by Dr. Samir
B. Pancholy from USA at the beginning, the 1st case of live
demonstration was televised from later than 9:30 AM. Tejas
did one case. The 1st case for me was a 60++ years old male
patient. He had a critical lesion in the proximal LAD and
a CTO in the middle RCA. The proposed plan of PCI was only
touching the LAD lesion. I did direct stenting using a Cypher
for LAD and tried to open the middle RCA lesion. Although
a Magic-S guidewire crossed the lesion, any balloon catheter
could not cross the lesion because of heavy calcification.
Because there were not so many resources, I gave up PCI
for this RCA.
| |
|
Tejas doing a
Case |
Doing a Case |
Next case had 2 CTO both in LAD and RCA. I
again used Magic guidewires. I am sure that they really
knew how Magic guidewires worked nicely for CTO lesions
especially with calcification.
During lunch time between 13:30 and 14:15, Tejas took me
to the meeting venue, which was an auditorium within NIRMA
University. This University is mainly for technology, pharmacy
and management, and established by the biggest soap company
in India in the suburb area of Ahmedabad. The campus of
the university is very huge. It is about 18 Km between the
auditorium and Sterling Hospital. An optical fiber network
was set up for this meeting for bi-directional transmission.
Image during live transmission was reported to be very clear,
although I had no chance to see it by me. A satellite network
was also reserved in case of the failure in an optical network.
The lunch was served in the field in front of the auditorium.
I was surprised to see one of my friends in Korea, Professor
Yoon from Wonju. After we finished lunch, I and Tejas came
back to the hospital. I did one case in the afternoon.
| |
|
|
NIRMA University |
Live Case Transmission |
With Dr Yoon |
Dr. Kan did one lecture about the hemostasis
devices for transradial approach. We came back to the hotel
around 6:00 PM. The state of Gujarat is a very religious
state, where any alcoholic beverages are not approved. We
cannot have them even within the hotels. However, we took
several bottles of alcohol beverages from Japan, and had
a small drinking party together with Ferdinand, Johan, Samir
and my Japanese colleagues.
| |
|
|
Drinking in the
Room |
Drinking with
Ferdinand |
With Tejas, Ferdinand,
John and Samir |
After finishing private drinking party, we
moved to the venue of welcome reception, which was one of
the farmer's gardens. All of the attendants joined this
outside dinner party.
January 22 Saturday, 2005
After finishing breakfast, I moved to Sterling
Hospital. In the morning of that day, I did 3 cases. One
of them was very serious. He was 50++ old male patient and
had class IV angina. The diagnostic coronary angiograms
showed total occlusions in LAD and RCA. He looked very serious.
After making the radial artery puncture, his blood pressure
dropped below 40 mmHg with slowed heart rate. Everybody
in the catheter laboratory as well as the audience thought
the mal condition happened due to the vagal reflex. I asked
to give intravenous atropine. However, although his heart
rate was increased after the injection of atropine, his
blood pressure did not increase over 40 mmHg. We started
intravenous catecholamine injection. Several moderators
suggested me to put IABP or even send to emergency coronary
artery bypass surgery. However, I thought that, if I could
open the occluded LAD, patients' condition would improve.
Thus, I continued the procedure. The engagement of the guiding
catheter into LCA was quite difficult. Finally, I could
engage a VL 3.0 guiding catheter into LCA. Since the patient's
hemodynamic status was really serious, I was also very serious
to do the procedure. I passed the total occlusion in the
proximal LAD by using a Magic-FA guidewire and placed a
drug-eluting stent in the lesion finally. After this treatment,
the patient's hemodynamic condition was stabilized.
During the 2 days' live transmission, I used
several kinds of drug-eluting stents. One of them was made
in India and packed in Germany. That is a Sirolimus-eluting
stent and already approved by EU Government. This stent
is imported from Germany to India. However, its price is
very low compared to Cypher. I used this stent several times.
Its trackability was very nice.
The live case transmission of that day was finished by noon.
My Japanese colleagues came to the hospital and had lunch
together. Cooking people in the hospital know well about
my preference on taste. They served a special dish for me.
That was flied green pepper. Curry for me was also well-seasoned
by hot pepper.
After having lunch, we moved to the meeting
venue. There, we had interviews from TV stations and newspapers
. Since we had finished live case transmission, we became
a little relaxed. We congratulated each other for the successful
live transmission. In the afternoon, we had case presentations
by doctors from India and Japan. I chaired the session of
case presentation with Tejas, Ferdinand and Samir. Still
there were a lot of attendants. Dr Masutani and Dr Sakai
did presentations. They did very nicely their jobs.
| |
|
Press Interview |
TV Interview |
| |
|
John, I, Ferdinand
and Tejas |
From the Stage |
The 1st TRICO meeting had finished with a
great success. The attendants exceeded 350 people, and most
of them were young Interventional Cardiologists from all
around India.
Before leaving the meeting venue, our Japanese team took
memorial photography together for this great success.
| |
Group Photo of
Japanese Colleagues |
On the night, we were invited to the big farm
owned by the president of the hospital. We had a wonderful
outside dinner there. There were several beautiful horses.
Also, there were several valuable antiques including an
old coach and a real sword.
| |
With John, Yoon
and Horse |
| |
|
Farm Dinner Party |
With a Horse |
| |
|
On the Coach
with John |
Real Sword |
We returned to the hotel around 11:00 PM.
January 23 Sunday, 2005
We waked up early and checked out the hotel
around 4:30 AM to leave Ahmedabad by taking a flight to
Singapore by SQ461 departing at 6:30 AM. I bade farewell
to my Japanese colleagues at Singapore Changi International
Airport. I had to attend the 14th Singapore Live Demonstration
Course, and they returned to Japan. I really appreciate
their attendance to TRICO 2005 meeting and congratulate
for their great success during their 1st trip to India.
インド訪問記IV
湘南鎌倉総合病院 心臓センター循環器科
副院長・部長 齋藤 滋
はじめに
私は、アーマダバードで私のインド最大の友人であるTejas Patel先生と共に、TRIのライブデモンストレーションを行うことを考えていました。世界の何処でもそうですが、TRIはインドでもどんどん盛んになりつつあります。しかし、インドでも比較的経験を積み、既に地位の確立した医者の間ではTRIに対する根強い反発があります。何回かTejasと打ち合わせ、2005年の1月に開催することを聞けました。この学会の名前はTRICO
2005と言います。TRICO 2005とは“Trans Radial Intervention COurse
2005”のことです。私はTejasと共に会の開催者であり、またオランダからKiemeneij先生、そしてアメリカのCoppola先生も招きました。今回、私は日本からRadialistとして、遠山先生、菅先生、坂井先生、舛谷先生、羽田先生そして部下の竹谷先生を招きました。
| |
|
TRICO Program
1 |
TRICO Program
2 |
成田空港に皆集合し、2005年1月20日木曜日の11:45 AM発クアラ・ルンプール(KL)行きJL723便に乗りました。飛行機はマレーシア時刻6:30
PM頃にクアラ・ルンプール国際空港に到着しました。すぐにアーマダバード行きのマレーシア航空MH178便に乗り継げる筈だったのですが、飛行機の出発は約1時間遅れました。このため、ラウンジで2時間ぐらいブラブラしていました。新しいKL国際空港はとても快適です。そこでは無線LANにより自由にラップトップをインターネットに接続することができます。KLが5時間ぐらいかけてアーマダバード国際空港に到着したのは現地時刻で翌日の午前0時でした。私たちはバスに乗ってプライド・ホテルに向かいました。ホテルに着いたのは午前0:30になっていました。時差がありますので、日本時刻では午前4:00ということになります。部屋に入ってからインターネット接続を探しましたが見つかりませんでした。そこでフロントから人を呼んだのですが、残念なことにこのホテルではインターネット高速接続は不可能でした。
ホテルはアーマダバード市内の中心にあります。部屋の窓から隣接するとてもお金持ちの家を見ることができました。
2005年1月21日金曜日
日本との3時間半の時差のせいでまたしてもひどい時差ぼけになってしまいました。1時間おきに目を覚ましました。そして、朝の5:30、日本時刻9:00AMに起床しました。
それからコンピューターで少し仕事しました。7:00 AMに朝食をとってから8:15 AMにSterling病院に向かいました。ここにはカテ室が二つあります。片方にはSiemens社製のフラット・パネルがあり、他方はPhilipsのH-5000です。カテ室にはたくさん医者、看護師、技師そしてTVスタッフがいました。皆緊張しているように見えました。
| |
|
|
Sterling Hospital |
Everybody in
Labo? |
TV Settings |
朝8:45からTejasの歓迎の言葉で会が始まる手筈でしたが、開始は少し遅れました。そして、引き続いてSamir
Pancholy先生による講義が入りましたので、一例目のライブ症例が実際に放映されたのは9:30 AMぐらいになっていました。Tejasが一例行いました。そして私が私の第一例目を行いました。患者さんは60歳台の男性患者さんでした。LADにきつい狭窄があり、右冠動脈にはCTOがありました。言われていたプランはLADにだけ治療する、というものでしたが、私はLADにCypherステントを直接植え込んだ後、そのまま右冠動脈のCTOを開けにかかりました。Magic-Sガイドワイヤーで病変を通過しましたが、石灰化がひどくどんなバルーンも病変を通過することができませんでした。あまり選択できる手段も無いので、この病変は諦めることとしました。
| |
|
Tejas doing a
Case |
Doing a Case |
次の症例はLADと右冠動脈の両方にCTO病変がありました。私は再度Magicガイドワイヤーを使いました。皆、MagicガイドワイヤーがCTO、特に石灰化を伴うCTOに対してすばらしいガイドワイヤーである、ということを良く実感できたことと思います。
午後1:30から2:15までの昼食時間の間にTejasは私を学会場に連れて行きました。会場はNIRMA大学講堂でした。この大学は主として工学、薬学そして経営学のための大学であり、インド最大の石鹸会社がアーマダバード郊外に設立したものです。とても広い大学キャンパスがあります。大学と病院は18
Km離れています。画像は光ファイバーで相方向に伝送されました。私は見ることができませんでしたが、会場の中継画像はとても美しいものだったそうです。また、バック・アップとして衛星も確保したそうです。昼食は講堂前の広場で行われました。韓国の友人Yoon先生に会って驚きました。昼食を終えてからTejasと私は病院に戻りました。午後もう一例私はしました。
| |
|
|
NIRMA University |
Live Case Transmission |
With Dr Yoon |
菅先生は経橈骨動脈穿刺後の止血器具の講義をされました。ホテルには夕方6時頃に戻りました。グジャラート州はとても敬虔な州です。酒類は一切禁止です。ホテルの中ですら飲むことが取り寄せることができないのです。でも、日本から何本かのお酒を持ち込んでいましたので、Ferdinand,
John, Samirそして日本の仲間と共に部屋で小さなパーティーを行いました。
| |
|
|
Drinking in the
Room |
Drinking with
Ferdinand |
With Tejas, Ferdinand,
John and Samir |
この秘密のパーティーの後、皆揃って農園で開催された歓迎式典に参加しました。屋外夕食会を皆楽しみました。
2005年1月22日土曜日
朝食後、Sterling病院に向かいました。その日の午前中私は三例行いました。この中の一例はとても重症の患者さんでした。患者さんは50歳台の男性患者さんでCCS
class IVの重症狭心症でした。診断カテーテルの結果、LADとRCAが完全閉塞でした。とても重症に見えました。橈骨動脈を穿刺すると徐脈と共に血圧が40
mmHg以下に低下してしまいました。カテ室の皆、そして会場の皆、この状況は迷走神経反射によるものだと思いました。私はアトロピンを投与するように命じました。しかし、アトロピン投与によって心拍数は回復したのですが、血圧は40
mmHg以下でした。そこでカテコラミンの投与も開始しました。会場のモデレーター何人かは私に、大動脈内バルーン・パンピングを入れるように、とか緊急冠動脈バイパス手術に回すべきだ、とか言いました。しかし、LADの閉塞を再開通させれば状態は改善する筈だ、と考えました。左冠動脈にガイディング・カテーテルを挿入するのはとても困難でした。VL
3.0ガイディング・カテーテルを用いてやっとのことで左冠動脈にガイディング・カテーテルを挿入することが出来ました。患者さんの血行動態状態は非常に深刻でしたので、私も非常に真剣に手技を行いました。Magic-FAガイドワイヤーを用いることによってLAD近位部の閉塞病変を通過できました。そして薬剤溶出性ステントを植え込みました。これによって患者さんの状態は安定しました。
この2日間のライブ中継で私は何種類の薬剤溶出性ステントを用いました。その中の一つはインドで製造され、ドイツで梱包されているものでした。このステントはシロリムス溶出性ステントであり、CEマークも取得しています。ドイツからインドに輸入されているのですが、Cypherと比較して価格は安いのです。何回かこのステントを用いましたが、とても良いステントです。
この日のライブ中継は昼で終了しました。日本からの先生方も病院に来られていましたので一緒に昼食を摂りました。この病院の食事係の人達は私の好みを分かっているので、私用に特別に用意してくれました。それが緑唐辛子を揚げたものです。私用のカレーも辛くしてありました。
昼食を終了して、我々は会場に移動しました。そこではテレビや新聞の会見が行われました。ライブ中継を終えたので、皆か少しリラックスしました。そして、互いにライブの成功を祝いました。午後は、私、Tejas,
FerdinandそしてSamirでインドと日本からの症例紹介のセッション座長を行いました。まだ会場にはたくさんの人がいました。舛谷先生と坂井先生も症例紹介を行いました。彼らはとてもうまく行いました。
| |
|
Press Interview |
TV Interview |
| |
|
John, I, Ferdinand
and Tejas |
From the Stage |
第一回TRICOは大成功に終わりました。参加者は350名を超え、そのほとんどがインドの各地から集まった若い循環器医師でした。
会場を去る前に、日本から参加された先生方と共にこの成功を祝って記念写真を撮影しました。
| |
Group Photo of
Japanese Colleagues |
その晩は、病院理事長が所有する牧場に行きました。そこでとてもすばらしい夕食会を持ちました。この牧場には美しい馬が何頭もいます。さらに、貴重な骨董品もあります。その中には、古い馬車そして本当の剣がありました
| |
With John, Yoon
and Horse |
| |
|
Farm Dinner Party |
With a Horse |
| |
|
On the Coach
with John |
Real Sword |
私たちは11:00頃ホテルに戻りました。
2005年1月23日 日曜日
我々は朝早く起床し、4:30 AM頃にはホテルをチェック・アウトしました。そして、6:30
AM発のSQ461便でシンガポールに向かいました。シンガポール・チャンギ国際空港で私は皆と別れを告げました。私は、第14回シンガポール・ライブデモンストレーションに参加せねばなりませんし、彼らは日本に帰国しました。彼らがTRICO
2005に参加されたことに本当に感謝します、そしてこの彼らにとっての初めてのインド旅行での大成功を祝したいと思います。
|